Introduction
Evolution of Medicine
- Humans have long attempted to control and relieve disease using available knowledge and practices.
- Early healers used observation, experience, and traditional remedies in the absence of scientific understanding.
- These early practices contributed to the gradual development of medical knowledge.
- Medical knowledge has evolved from accumulated observations, practical experiences, and critical analysis over time.
- The history of medicine includes both successful discoveries and incorrect theories that were later corrected.
- It reflects the progressive growth of human understanding, scientific thinking, and healthcare practices.
Sources of Medical Advancement
- Medicine developed in stages, with periods of progress and stagnation.
- Early medicine was strongly influenced by cultural traditions and empirical practices.
- Later advancements were driven by biological sciences and natural sciences.
- More recently, social and behavioural sciences have influenced medical practice and public health approaches.
- Modern medicine integrates knowledge from multiple disciplines to improve healthcare delivery.
Modern Medicine and Challenges
- Medicine has become a complex system influenced by administrative and policy structures.
- Rapid expansion of scientific knowledge has increased the complexity and cost of treatment.
- Access to modern healthcare remains uneven across populations and regions.
- Significant disparities exist between developed and developing regions, and between urban and rural populations.
- These inequalities are recognized as major issues of health equity and social justice.
Goals of Contemporary Medicine
- Global efforts aim to reduce inequalities in healthcare access and resource distribution.
- International initiatives focus on achieving Sustainable Development Goals related to health.
- The scope of medicine has expanded beyond treatment to include disease prevention.
- Emphasis is placed on health promotion and improving overall quality of life.
- Medicine is now considered a key component of socio-economic development and community well-being.

Medicine in Antiquity
- In ancient periods, concepts of health and illness were explained using cosmological and human-centered beliefs.
- Medical practices were closely linked with religion and supernatural interpretations.
- Healing methods often included rituals, spiritual practices, and traditional remedies.
- These approaches reflected the cultural and intellectual environment of early societies.
Relationship with Culture and Society
- Every civilization developed its own system of medicine based on its beliefs and experiences.
- Medical practices were shaped by prevailing cultural, social, and environmental conditions.
- Medicine played a role in unifying communities and supporting early societal organization.
- It contributed to the gradual development of scientific thinking and organized knowledge.
Influence of Broader Factors
- The understanding of disease was influenced by philosophy, religion, and available knowledge systems.
- Economic conditions and forms of governance affected access to healthcare and treatment methods.
- Educational systems and scientific progress influenced how diseases were interpreted and managed.
- Medical practices must be understood within the broader context of human development and societal evolution.
Primitive medicine
- Early humans provided care out of sympathy and the need to relieve suffering.
- Caregiving roles emerged naturally within families and communities.
- Limited knowledge led to non-scientific explanations for illness and suffering.
Supernatural Concepts of Disease
- Disease was explained by the supernatural theory of disease.
- Illness was attributed to divine punishment, evil forces, or cosmic influences.
- These beliefs shaped early approaches to diagnosis and treatment.
Methods of Treatment
- Treatment methods included prayers, rituals, and sacrifices to appease perceived supernatural forces.
- Practices such as exorcism, use of charms, and protective amulets were common.
- Herbal substances were administered, although their effects were often uncertain.
- Early surgical procedures, including trephination, amputations, and circumcision, were performed using simple tools made of stone or flint.
Characteristics of Primitive Medicine
- Medicine during prehistoric periods, around 5000 before the Common Era, was closely associated with religion, magic, and superstition.
- Practices were based on belief systems rather than scientific evidence.
- Knowledge was transmitted through tradition and experience.
Persistence in Modern Times
- Elements of primitive medicine still exist in various regions of the world.
- Some communities continue to use traditional healing methods based on cultural beliefs.
- Misinterpretation of diseases, such as linking illness to past actions, persists in certain settings.
- Traditional healers remain accessible and are often trusted within local communities.
- Some traditional practices may delay access to evidence-based medical care.
Indian Medicine
- The Ayurveda and Siddha systems are the principal indigenous medical traditions of India.
- Ayurveda is practiced widely across India, whereas the Siddha system is mainly followed in Tamil-speaking regions of South India.
- Both systems share similar theoretical foundations and clinical approaches, with only minor variations in practice.
- Ayurveda refers to the “knowledge of life” emphasizing the maintenance, promotion, and prolongation of health.
- Its origins can be traced to ancient Vedic literature, about 5000 B.C., indicating development over several millennia.
- Early medical concepts were closely linked with philosophical and spiritual traditions.
- As a result of the churning of the oceans during a “tug of war” between gods and demons, Dhanvantari, the Hindu god of medicine is said to have been born
- The Atharvaveda contains early descriptions of health, disease, and therapeutic measures, forming a basis for later systematic medical knowledge. Over time, these concepts evolved into a structured and comprehensive medical system with defined principles and practices.
Development of Ayurveda in Ancient India
- Atreya (800 B.C.) is regarded as one of the earliest Indian physicians and teachers of Ayurveda.
- He was associated with the ancient center of learning at Takshashila, located near present-day Rawalpindi.
- Ayurveda expanded significantly during the Buddhist period, receiving organized support and wider acceptance.
- King Ashoka (226 B.C.) promoted Ayurveda as state-supported medicine and established medical schools and hospitals.
Contributions of Classical Texts and Physicians
- Charaka (200 A.D.), a court physician to the Buddhist king Kanishka, based on Atreya’s teachings systematized medical knowledge in the Charaka Samhita.
- He describes approximately 500 medicinal substances derived from plants, minerals, and animal sources.
- Physicians used Rauwolfia serpentina (Indian snakeroot) for centuries before the isolation of reserpine for treating hypertension.
Surgical Advancements
- Sushruta, “father of Indian surgery” compiled surgical knowledge in the Sushruta Samhita, dated between 800 B.C. and 400 A.D.
- The text includes detailed information on surgery, anatomy, pathology, obstetrics, ophthalmology, and hygiene.
- Early practitioners performed procedures such as fracture management, amputations, tumour excision, hernia repair, cataract surgery, and plastic surgery.
- It is reported that during the period of the East India Company, British physicians acquired the technique of rhinoplasty from Indian surgeons.
Decline of Surgical Practice
- Surgical progress declined during the Buddhist era due to the emphasis on ahimsa (non-violence), which discouraged invasive procedures.
Tridosha Theory of Disease
- Ayurveda is based on the tridosha theory, which explains health and disease through three fundamental biological principles.
- The three doshas or humors are vata (wind), pitta (gall) and kapha (mucus).
- Health is defined as a state of equilibrium among the three doshas.
- Disease occurs when there is a disturbance or imbalance in one or more doshas, affecting normal physiological functions.
- The tridosha concept shows similarity to the four-humor theory described in ancient Greek medicine.
Exchange of Medical Knowledge
- There was active intellectual exchange among Hindu, Arab, Persian, Greek, and Jewish scholars in ancient and early medieval periods.
- The classical Ayurvedic texts, including the Charaka Samhita and Sushruta Samhita, were translated into Persian and Arabic around 800 A.D.
- These translations facilitated the spread of Ayurvedic knowledge beyond India and contributed to the development of other medical traditions.
Hygiene in Ancient Indian Medicine
- Hygiene was considered an essential component of health in ancient Indian medical practice.
- The Laws of Manu provided structured guidelines on personal cleanliness, diet, and daily conduct.
- These regulations emphasized routine practices such as bathing, sanitation, and disciplined lifestyle habits.
Archaeological Evidence
- Excavations at Mohenjo-daro and Harappa in the Indus Valley revealed urban settlements dating to approximately 2600–1900 B.C.
- The cities demonstrated well-planned drainage systems, public baths, and organized water supply.
- These findings indicate advanced knowledge of sanitation engineering and public health measures for that period.
Growth and Decline of Ayurveda
- The classical or golden period of Ayurveda extended from 800 B.C. to 600 A.D.
- During this time, systematic medical texts, clinical methods, and surgical practices were well developed.
- Ayurveda experienced a decline during the Mughal period and subsequent centuries due to reduced institutional and state support.
Influence of Indian Medicine in Asia
- Medical historians recognize that Indian medicine had a major influence across Asia, comparable to the role of Greek medicine in the West.
- It spread to regions such as Indochina, Indonesia, Tibet, Central Asia, and Japan. This diffusion reflects the transmission of medical knowledge through trade, cultural exchange, and scholarly interactions.
Unani-Tibb System of Medicine
- Unani-Tibb is an indigenous system in India, although its origin lies in ancient Greek medicine.
- It was introduced into India by Muslim rulers around the 10th century A.D.
- By the 13th century, it became established in major centers such as Delhi, Aligarh, Lucknow, and Hyderabad.
- The system received continuous state patronage under successive Muslim rulers until the advent of British rule in the 18th century.
Homoeopathy
- Homoeopathy was developed by Samuel Hahnemann (1755–1843) in Germany.
- It gained acceptance in India between 1810 and 1839.
- The system is based on the principle of “similia similibus curentur” (like cures like).
- It uses small doses of substances that produce symptoms similar to the disease in healthy individuals.
- India currently has one of the largest numbers of homoeopathic practitioners globally.
Contemporary Relevance
- Indian systems of medicine, including Ayurveda, Unani-Tibb, and Homoeopathy, remain widely practiced.
- These systems form an integral part of Indian cultural and healthcare traditions.
- They continue to provide accessible medical care, particularly to rural populations.
Chinese medicine
- Chinese medicine is regarded as one of the earliest organized medical systems, with origins traced to around 2700 B.C.
- It is founded on the philosophical concept of yin and yang, representing two opposing yet complementary forces.
Principles of Yin and Yang
- Yang is considered the active, dynamic, and masculine principle.
- Yin is regarded as the passive, receptive, and feminine principle.
- Maintenance of a balanced interaction between yin and yang was believed to be essential for health.
- Disease was interpreted as a disturbance in this equilibrium.
Preventive and Therapeutic Practices
- Chinese physicians emphasized preventive care alongside treatment.
- Common methods included:
- Hygiene practices to maintain cleanliness and prevent disease.
- Dietetics, focusing on balanced nutrition.
- Hydrotherapy, involving the therapeutic use of water.
- Massage therapy to improve circulation and relieve symptoms.
- Use of medicinal drugs, often derived from natural sources.
Early Immunization Practices
- The Chinese were among the first to develop immunization techniques.
- They practised variolation to prevent smallpox, an early form of protective inoculation.
Medical Philosophy and Public Health
- A key principle stated “the great doctor is one who treats not someone who is already ill but someone not yet ill”.
- Traditional Chinese medicine remains widely trusted and is integrated with modern medical systems.
Notable Contributions
- The concept of “barefoot doctors” improved rural healthcare delivery, especially in the 20th century.
- Techniques such as acupuncture have gained global recognition for their therapeutic applications.
Egyptian medicine
- Ancient Egypt was one of the earliest civilizations, flourishing around 2000 B.C.
- Knowledge about this period is extensive due to hieroglyphic writing recorded on papyrus manuscripts.
Medicine and Religion
- Medical practice was closely associated with religious beliefs.
- Physicians often held positions equal to priests and were trained in temple-based schools.
- Patients were frequently treated in temples, where both spiritual and physical care were provided.
Anatomical Knowledge and Limitations
- There were no systematic anatomical dissections because religious beliefs required preservation of the body after death.
- This restriction limited the development of anatomical science, although practical medical skills were still applied.
Contributions and Key Figure
- Egyptian medicine reached a high level during the time of Imhotep (2800 B.C.).
- Imhotep was known as a physician, architect, and statesman, and he designed the step pyramid at Saqqarah.
- He was later regarded as both a healer and a deity, reflecting the integration of medicine and religion.
Medical Practice and Specialization
- A notable feature was the presence of medical specialization.
- Distinct practitioners included:
- Eye specialists
- Head specialists
- Dental practitioners
- Physicians were often state-appointed officials and received compensation from the government.
Historical Recognition
- Ancient Egyptian physicians were highly regarded in antiquity.
- The poet Homer described them as “the best of all”, indicating their reputation in the ancient world.
Concepts of Disease and Physiology
- Egyptian medicine was systematic and advanced, not primitive.
- Disease was believed to result from harmful substances absorbed from the intestine, leading to putrefaction of blood and formation of pus.
- The pulse was considered the “speech of the heart,” indicating an early attempt to relate circulation with clinical signs.
Therapeutic Practices
- Treatment methods were diverse and included:
- Cathartics to promote bowel evacuation.
- Enemas for intestinal cleansing.
- Blood-letting to remove impure blood.
- Use of a wide range of medicinal substances derived from plants and minerals.
Important Medical Texts
- Two major Egyptian medical manuscripts are documented:
- Edwin Smith papyrus (3000–2500 B.C.):
- Recognized as the earliest known surgical text.
- Describes clinical conditions such as partial paralysis following cerebral injury in skull fractures with notable accuracy.
- Ebers papyrus (1150 B.C.):
- Was found with a mummy on the banks of the Nile,
- Contains approximately 800 prescriptions based on around 700 drugs.
- Provides unique extensive information on pharmacological practices.
- Edwin Smith papyrus (3000–2500 B.C.):
Drugs and Materia Medica
- Egyptian physicians used a variety of substances, including:
- Castor oil, tannic acid, opium, and turpentine.
- Plant-based drugs such as gentian and senna.
- Mineral compounds and root-derived preparations.
Diseases Described in Papyri
- The papyri document several diseases, including:
- Parasitic infections (worms)
- Eye disorders
- Diabetes mellitus
- Rheumatic conditions
- Poliomyelitis
- Schistosomiasis
- Many of these conditions continue to be public health concerns in modern Egypt.
Public Health Achievements in Ancient Egypt
- Ancient Egyptians demonstrated advanced understanding of public health practices.
- They developed planned urban settlements with organized layouts.
- Infrastructure included public baths and underground drainage systems, indicating attention to sanitation and hygiene.
Preventive Health Measures
- There is evidence suggesting early awareness of inoculation-like practices against smallpox (though systematic variolation developed later).
- The use of mosquito nets indicates recognition of insect-related disease prevention.
- Egyptians associated plague with rats, reflecting an early observation of disease transmission patterns.
Religion and Health
- The Egyptian god of health was Horus.
- Religious beliefs continued to influence both preventive and therapeutic practices.
Historical Significance
- Egyptian medicine held a dominant position in the ancient world for nearly 2,500 years.
- It was later superseded by Greek medicine, which introduced more systematic theoretical approaches.
Mesopotamian medicine
- Mesopotamian civilization developed alongside ancient Egypt, in the region between the Tigris and Euphrates rivers (present-day Iraq).
- It is often referred to as the “Cradle of Civilization”, with origins dating back nearly 6,000 years.
Concepts and Practice of Medicine
- Medical knowledge was largely influenced by religious and supernatural beliefs.
- Practitioners were classified into three groups:
- Herb doctors, who used plant-based remedies (similar to physicians).
- Knife doctors, who performed surgical procedures.
- Spell doctors, who managed illnesses attributed to supernatural causes.
- This classification broadly resembles modern divisions such as internal medicine, surgery, and mental health care.
Beliefs About Disease
- Diseases were often attributed to demons or supernatural forces.
- Medical training involved identifying and classifying these perceived causes.
- Practices such as geomancy and dream interpretation were used for diagnosis.
- Hepatoscopy (examination of the liver) was common, as the liver was considered the seat of life.
Medical Literature and Records
- Medical knowledge was documented on clay tablets using cuneiform script.
- The oldest known medical prescription dates to approximately 2100 B.C.
Contributions to Medical Thought
- Civilizations such as the Sumerians, Babylonians, and Assyrians contributed to the development of medical astrology.
- These ideas influenced medical traditions across Eurasia for many centuries.
Code of Hammurabi and Medical Regulation
- Hammurabi, the king of Babylon, lived around 2000 B.C. and established a formal legal system.
- He introduced the Code of Hammurabi, one of the earliest known legal codes governing medical practice.
Regulation of Physicians
- The code clearly defined the conduct and responsibilities of physicians.
- It specified fees for successful treatment, indicating regulated medical remuneration.
- It also prescribed strict penalties for unsuccessful or harmful treatment.
- In severe cases, physicians could face capital punishment if their treatment caused harm.
Significance of the Code
- The code represents the first known codification of medical ethics and practice.
- It reflects a high level of social organization and administrative control over healthcare.
Scientific Limitations
- Despite legal regulation, medical practice during this period lacked a scientific foundation.
- Diagnosis and treatment were still largely influenced by supernatural beliefs and empirical observations rather than systematic scientific methods.
Greek medicine
- The classical period of Greek medicine extended from 460–136 B.C.
- Greek civilization was influential in promoting rational thinking, emphasizing explanations based on “why” and “how” rather than superstition.
Early Figures and Mythological Influence
- An early figure in Greek medicine was Asclepius (around 1200 B.C.), regarded as a deity of healing.
- His daughters played symbolic roles:
- Hygieia was worshipped as the goddess of health.
- Panacea as the goddess of medicine.
Development of Medical Philosophy
- The traditions associated with Hygieia and Panacea led to two approaches:
- Preventive medicine, focusing on maintenance of health.
- Curative medicine, focusing on treatment of disease.
- This distinction represents an early conceptual division in medical practice that continues in modern healthcare systems.
Symbolism and Legacy
- The symbol of Rod of Asclepius, a staff with a serpent entwined around it, remains an enduring emblem of medicine.
- Greek medicine laid the foundation for a more systematic and rational approach to health and disease.
Historical Interpretation
- The ideas of prevention versus cure continue to influence modern public health and clinical medicine.
- Preventive approaches (associated with Hygieia) are increasingly emphasized, although curative care (associated with Panacea) continues to receive substantial resources.
Life and Background
- Hippocrates ( 460–370 B.C. ) is widely regarded as the “Father of Medicine”.
- He was born around 460 B.C. on the island of Cos in the Aegean Sea.
Contributions to Medical Science
- He introduced a systematic and rational approach to medicine based on observation and reasoning.
- Diseases were studied and classified using clinical features, rather than supernatural explanations.
- He rejected the dominance of magic and superstition, promoting clinical methods in diagnosis and treatment.
Corpus Hippocraticum
- His teachings were later compiled by Alexandrian scholars into the “Corpus Hippocraticum”.
- This collection consists of about 72 volumes covering various branches of medicine.
- It includes some of the earliest scientific clinical case records, forming a basis for clinical practice.
Ethical Principles
- The Hippocratic Oath established a code of medical ethics.
- It emphasizes professional integrity, confidentiality, and responsibility towards patients.
- The oath remains a foundational influence on modern medical ethics.
Philosophical Insights
- Notable sayings attributed to Hippocrates include:
- “Life is short, the art long, opportunity fleeting, experience uncertain, and judgment difficult.”
- “Where there is love for mankind, there is love for the art of healing.”
Significance
- Hippocrates laid the foundation for scientific medicine and clinical practice.
- He is recognized as one of the most influential figures in the history of medicine.
Hippocrates and Early Epidemiology
- Hippocrates ( 460–370 B.C. ) made important contributions to epidemiology.
- He distinguished between epidemic diseases (occurring in outbreaks) and endemic diseases (persistently present in a population). This classification represents one of the earliest systematic approaches to studying disease distribution.
Study of Disease Determinants
- He emphasized identifying the causes of disease through observation.
- Factors examined included:
- Climate and seasonal variations
- Water quality
- Dietary patterns
- Clothing and living habits
- These observations highlighted the role of environmental and lifestyle factors in disease occurrence.
“Airs, Waters and Places”
- His work “Airs, Waters and Places” is considered an early text on social medicine and hygiene.
- It systematically relates environmental conditions to patterns of disease in communities.
Concept of Health and Disease
- The Hippocratic view defined health as a balance between humans and their environment.
- Disease was interpreted as a result of disturbance in this relationship, rather than supernatural causes.
Significance
- These ideas laid the foundation for modern concepts of public health and preventive medicine.
- Hippocrates is therefore regarded as one of the earliest contributors to scientific epidemiology.
Shift in Medical Thought
- Greek medicine introduced a rational and naturalistic approach to disease.
- Diseases were explained as natural processes, not as consequences of supernatural forces or divine punishment.
Theory of Elements and Humors
- Greeks proposed that all matter consists of four elements: earth, air, fire, and water.
- Each element was associated with qualities:
- Cold, dry, hot, and moist.
- These corresponded to four bodily humors:
- Phlegm
- Yellow bile
- Blood
- Black bile
- This framework is conceptually comparable to the tridosha theory in Ayurveda.
Concept of Health and Disease
- Health was believed to depend on the equilibrium of the four humors.
- Disease occurred when this balance was disturbed.
- The body was considered to possess an intrinsic ability to restore balance.
Role of the Physician
- The physician’s primary function was to support natural healing processes.
- Treatment aimed to restore humoral equilibrium rather than merely suppress symptoms.
Scientific Perspective and Relevance
- The humoral theory, although scientifically incorrect, represented an early attempt to explain disease systematically.
- The concept of the body’s self-regulating and adaptive capacity remains relevant in modern physiology and medicine.
Alexandria as a Medical Centre
- After the Hippocratic period, Alexandria emerged as a major centre of learning.
- Its museum and library are regarded as among the earliest forms of a university system.
- The library housed more than 70,000 books, reflecting extensive scholarly activity.
- Between 300 B.C. and 30 B.C., large numbers of students were trained in Alexandria.
- Alexandria gradually replaced Athens as the leading centre of knowledge.
Influence on Medical Traditions
- The Hippocratic school strongly influenced the development of the Alexandrian school.
- It also contributed to the growth of Arabo-Persian medicine in later centuries.
- This continuity ensured the preservation and transmission of Greek medical ideas.
Advancement of Scientific Medicine
- The Hippocratic tradition helped to separate medicine from magic and superstition.
- It established medicine as a rational and observational science.
- Although scientific methods were applied, detailed scientific knowledge remained limited.
Historical Transition
- The decline of Greek civilization led to a gradual shift in influence.
- It was followed by the rise of the Roman civilization, which carried forward aspects of Greek medical knowledge.
Roman medicine
- By the 1st century B.C., Rome became the centre of civilization and governance.
- Roman medicine was largely derived from Greek medicine, following their conquest of Greek territories.
- Although political power became Roman, medical knowledge remained predominantly Greek in origin.
- Roman ideology emphasized the supremacy of the State over the individual, influencing public health policies.
Public Health and Sanitation
- Romans were practical and engineering-oriented, with strong emphasis on sanitation and public health.
- Major contributions included:
- Construction of public baths to promote hygiene.
- Development of sewerage systems for waste disposal.
- Building of aqueducts to supply clean water to cities.
- These measures mark the early development of organized public health systems.
Infrastructure and Disease Control
- The Romans constructed extensive road networks, facilitating communication and healthcare access.
- They implemented drainage of marshes to reduce diseases such as malaria.
- Urban planning incorporated clean water supply and waste management, reducing environmental health risks.
Medical Care Facilities
- Romans established early forms of hospitals, particularly for soldiers and the sick.
- These institutions represent an important step toward organized healthcare delivery systems.
Significance
- Roman contributions laid the foundation for environmental sanitation and public health engineering.
- Their emphasis on preventive measures and infrastructure continues to influence modern public health practices.
Life and Background
- Galen ( 130–205 A.D. ) was a prominent medical teacher of the Roman era.
- He was born in Pergamon (Asia Minor, present-day Turkey).
- He served as physician to the Roman emperor Marcus Aurelius.
Scientific Contributions
- Galen made significant contributions to comparative anatomy and experimental physiology.
- His work advanced understanding of body structure and function through systematic observation and experimentation.
Concepts of Health and Disease
- He emphasized that health preservation precedes disease treatment.
- He stated that maintaining health should be the primary objective, followed by curing disease.
- Galen proposed that disease arises due to three factors:
- Predisposing factors
- Exciting factors
- Environmental factors
- This reflects an early multifactorial concept of disease causation.
Relation to Hippocratic Thought
- The teachings of Galen and Hippocrates differed in approach:
- Hippocrates followed a more synthetic (holistic) method.
- Galen applied a more analytical and experimental method.
Writings and Influence
- Galen authored approximately 500 medical treatises covering diverse topics.
- His works dominated medical knowledge and he was regarded as a “medical authority” for centuries.
- His teachings influenced European medicine for nearly 14 centuries.
Later Developments
- His views were later challenged by:
- Andreas Vesalius in 1543 (anatomy).
- William Harvey in 1628 (circulation of blood).
- These developments marked the transition toward modern scientific medicine.
Middle ages
- The period from 500 to 1500 A.D. is referred to as the Middle Ages.
- The fall of the Roman Empire led to the decline of organized medical institutions and schools.
Health Conditions and Diseases
- Europe experienced widespread epidemics and endemic diseases.
- Common diseases included:
- Plague
- Smallpox
- Leprosy
- Tuberculosis
- Poor living conditions contributed to the spread of infectious diseases.
Nature of Medical Practice
- Medical practice largely regressed and became influenced by superstition and religious dogma.
- There was reduced emphasis on scientific observation and rational inquiry.
- Spiritual beliefs often dominated explanations of health and disease.
Social and Cultural Influences
- The body was often viewed negatively, while spiritual life was emphasized.
- Personal hygiene practices declined, and bathing was infrequent in many regions.
- Human dissection was generally restricted, limiting progress in anatomical knowledge.
Scientific Progress
- Due to restrictions and prevailing beliefs, there was limited advancement in medical science.
- This period is often termed the “Dark Ages of Medicine” because of relative stagnation.
Historical Significance
- Despite setbacks, the era involved social and political transformations.
- It represents a phase of both regression and gradual transition, setting the stage for later medical revival.
Overview of Arabic Medicine
- During Europe’s Dark Ages (500–1500 A.D.), the Arab world advanced significantly in medicine.
- Scholars translated Graeco-Roman medical texts into Arabic, preserving and expanding ancient knowledge.
- They developed the Unani system of medicine, based largely on Greek and Roman principles.
Institutions and Medical Education
- Arabs established medical schools and hospitals in major cities such as Baghdad, Damascus, and Cairo.
- These institutions promoted organized teaching, clinical practice, and patient care.
Notable Physicians
- Rhazes ( 865–925 A.D. ):
- Served as a hospital director in Baghdad.
- Described pupillary reaction to light.
- Used mercurial compounds in therapy.
- Authored an early text on paediatric diseases.
- Distinguished smallpox and measles clinically.
- Avicenna ( 980–1037 A.D. ):
- Compiled the “Canon of Medicine” (21 volumes).
- Systematized medical knowledge and influenced practice for centuries.
- Played a key role in advancing Islamic medicine.
Contributions to Pharmacology
- Arabs made major advances in pharmacology and pharmaceutical chemistry.
- They introduced numerous herbal and chemical drugs.
- Developed methods for preparing:
- Syrups, oils, poultices, plasters
- Pills, powders, and aromatic waters
- They formalized the art of prescription writing, influencing modern pharmacy.
Terminology and Innovations
- Several medical terms have Arabic origins, including:
- Drug, alcohol, syrup, and sugar
Historical Significance
- The golden age of Arabic medicine (800–1300 A.D.) marked a peak in medical scholarship.
- Arab scholars acted as a bridge between ancient and modern medicine, preserving and transmitting knowledge to later European systems.
Influence of Christianity on Healthcare
- During the Middle Ages (500–1500 A.D.), Christianity contributed to the growth of organized care for the sick.
- The spread of Christianity encouraged the establishment of hospitals across Europe.
- Early hospitals mainly provided basic care and spiritual support, rather than specialized medical treatment.
Development of Hospitals
- One of the earliest hospitals in England was built in York in 937 A.D.
- With the expansion of medical practice, numerous hospitals were established from Persia to Spain.
- Historical records indicate:
- Over 60 hospitals in Baghdad
- Around 33 hospitals in Cairo
- Some advanced institutions, such as Al Mansur Hospital in Cairo, included:
- Separate wards for different diseases and for both sexes
- Facilities like cooling fountains for fever management
- Libraries, and provisions for music and storytelling to comfort patients
Role of Monasteries
- Religious institutions known as monasteries played a key role in healthcare delivery.
- They were managed by monks, abbots, and religious leaders.
- Monasteries admitted individuals from all social classes, including royalty.
- They helped preserve ancient medical knowledge and provided nursing and supportive care.
Significance
- These developments contributed to the early evolution of institutional healthcare systems.
- Although treatment remained limited, emphasis on care, compassion, and shelter laid the groundwork for modern hospitals.
DAWN OF SCIENTIFIC MEDICINE
- The period after 1500 A.D. marked the transition to scientific medicine.
- It was characterized by major political, industrial, religious, and medical changes.
- Political revolutions in France and America emphasized individual rights and social reform.
- The Industrial Revolution improved living standards, while also creating new health challenges.
- Medicine evolved with increasing reliance on observation, experimentation, and rational inquiry.
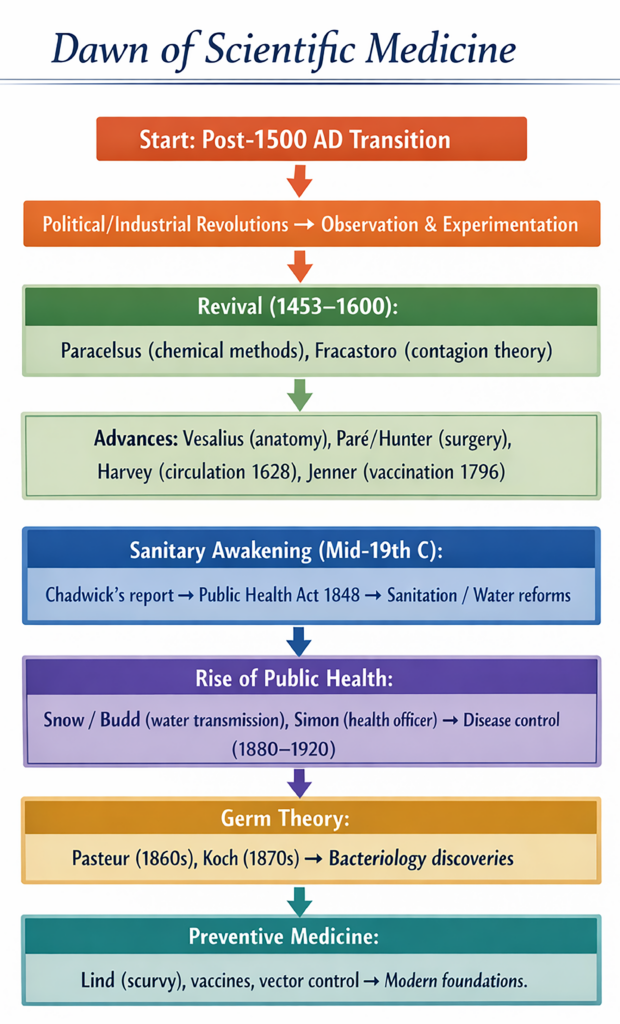
Revival of medicine(1453–1600 A.D.)
- The revival period from 1453–1600 A.D. represented an era of independent scientific investigation.
- It marked a shift from traditional authority to critical thinking in medical science.
Contributors
- Paracelsus ( 1493–1541 ):
- Challenged traditional teachings of Galen and Avicenna.
- Publicly rejected superstition and dogma in medicine.
- Promoted experimental and chemical approaches to treatment.
- Played a major role in redirecting medicine toward scientific research.
- Girolamo Fracastoro ( 1483–1553 ):
- Proposed the theory of contagion, explaining disease transmission.
- Suggested that infections spread through minute invisible particles.
- Identified person-to-person transmission of syphilis.
- Contributed to the early development of epidemiology.
Significance
- This period laid the groundwork for modern medical science.
- It emphasized causation, transmission of disease, and scientific reasoning, replacing earlier speculative beliefs.
Advances in Anatomy and Surgery
- Andreas Vesalius ( 1514–1564 ) conducted extensive human dissections and identified errors in Galen’s teachings.
- He established anatomy as a scientific discipline and authored Fabrica, a classic medical text.
- Ambroise Pare ( 1510–1590 ) advanced practical surgical techniques and is known as the “father of surgery”.
- John Hunter ( 1728–1793 ) later developed the scientific basis of surgery.
- In 1540, the United Company of Barber Surgeons was established in England, later evolving into the Royal College of Surgeons.
Clinical Medicine and Epidemiology
- Thomas Sydenham ( 1624–1689 ) emphasized the clinical method based on observation.
- He differentiated diseases such as scarlet fever, malaria, dysentery, and cholera.
- He is also regarded as an early epidemiologist.
Major Scientific Discoveries
- William Harvey discovered blood circulation in 1628.
- Antonie van Leeuwenhoek developed the microscope around 1670, enabling study of microorganisms.
- Edward Jenner introduced smallpox vaccination in 1796.
Foundation of Modern Pathology
- Giovanni Battista Morgagni ( 1682–1771 ) founded pathological anatomy.
- He correlated clinical symptoms with post-mortem findings, establishing a scientific basis for disease understanding.
Significance
- The 17th and 18th centuries marked rapid progress in medical science and surgery.
- These developments laid the foundation for the major advances of 19th century medicine.
Sanitary Awakening (Mid-19th Century)
- The “great sanitary awakening” began in England in the mid-19th century and later spread globally.
- It marked the beginning of organized public health reforms and changes in community behaviour.
Background: Impact of Industrialization
- The Industrial Revolution (18th century) led to rapid urbanization and major health problems:
- Formation of slums and overcrowding
- Accumulation of waste and poor sanitation
- Increased infectious diseases, including tuberculosis
- High morbidity and mortality, especially among women and children
- In 1842, the mean age at death in London was:
- 44 years among the gentry and professionals
- 22 years among the working class
Cholera and Public Health Crisis
- Recurrent cholera epidemics, especially the outbreak of 1832, worsened public health conditions.
- These epidemics highlighted the urgent need for sanitary reforms.
Role of Edwin Chadwick
- Edwin Chadwick ( 1800–1890 ) investigated urban health conditions.
- His report titled “The Sanitary Conditions of the Labouring Population in Great Britain” became a landmark document.
- It emphasized the relationship between poor sanitation and disease.
Public Health Reforms
- Chadwick’s work led to improvements in:
- Housing conditions
- Water supply and sanitation systems
- Urban environmental management
- The movement initiated an anti-filth campaign, recognizing filth as a major cause of disease.
Legislative Action
- The reforms resulted in the Public Health Act of 1848 in England.
- This act established a framework for government involvement in public health.
Significance
- A new principle emerged: the State is responsible for the health of its population.
- The sanitary awakening laid the foundation for modern public health systems and policies.
Rise of public health
- The modern concept of public health developed in England around 1840.
- Johann Peter Frank ( 1745–1821 ) earlier proposed that health is a responsibility of the State, enforced through laws.
- The Public Health Act of 1848 reflected this principle and marked a major policy shift.
Role of Epidemics
- Cholera, often termed the “father of public health”, recurred frequently in the 19th century.
- These epidemics highlighted the importance of environmental sanitation and safe water supply.
Contributions of Key Epidemiologists
- John Snow studied cholera outbreaks in London (1848–1854).
- He demonstrated that contaminated drinking water was responsible for disease transmission.
- William Budd ( 1856 ) showed that typhoid fever spreads through water contamination, not by miasma.
- These findings were significant despite the absence of identified microorganisms at that time.
Legislative and Environmental Reforms
- Growing public demand led to improved water supply and sanitation systems.
- The River Thames had served both as a drinking water source and sewage outlet, highlighting poor conditions.
- The Public Health Act of 1875 introduced comprehensive measures to control the physical environment.
Leadership in Public Health
- Sir John Simon ( 1816–1904 ), the first Medical Officer of Health in London, played a key role.
- He developed an effective public health system, which became a model for other countries.
Disease Control Phase (1880–1920)
- The early phase of public health (1880–1920) focused on disease control.
- Key measures included:
- Environmental sanitation and cleanliness
- Garbage and waste disposal
- Quarantine practices to prevent disease spread
- This period established the foundation for modern public health practice.
- It emphasized the importance of prevention, sanitation, and government responsibility in maintaining population health.
Public Health Development in America
- The growth of public health in America closely followed the English model.
- Lemuel Shattuck ( 1793–1859 ) published a landmark report in 1850 on health conditions in Massachusetts.
- His report, similar to Chadwick’s, emphasized the need for sanitation, data collection, and organized health systems.
- It played a key role in promoting public health reforms in the United States.
Expansion in Western Countries
- Countries such as France, Spain, Australia, Germany, Italy, Belgium, and Scandinavian nations developed structured public health systems.
- By the early 20th century, key foundations of public health were established:
- Clean water supply
- Improved environmental sanitation
- Healthy housing conditions
- Regulation of hazardous occupations and industries
Developments After World War I
- After World War I (1914–1918), countries like Yugoslavia, Turkey, and Russia began strengthening their public health systems.
- Around 1920, these nations had characteristics of underdeveloped regions, but later achieved significant progress in public health.
Global Disparities in Public Health
- While public health advanced rapidly in the Western world, progress remained slower in developing countries such as India.
- Many developing regions continued to face infectious diseases and sanitation issues similar to those seen in the West about 100 years earlier.
Role of International Organizations
- The establishment of the World Health Organization (WHO) strengthened global public health efforts.
- WHO introduced a Health Charter aimed at improving health standards worldwide.
Significance
- This period marked the global expansion of public health principles.
- It highlighted the importance of international cooperation, infrastructure development, and preventive strategies in improving population health.
Germ theory of disease
Early Theories of Disease
- Before modern science, several theories attempted to explain disease causation:
- Supernatural theory (divine or spiritual causes)
- Humoral theory (imbalance of bodily fluids)
- Contagion theory (person-to-person spread)
- Miasmatic theory (disease due to foul air and vapours)
- Spontaneous generation theory (life arising from non-living matter)
- These explanations lacked experimental validation.
Emergence of Germ Theory
- A major breakthrough occurred in 1860, when Louis Pasteur ( 1822–1895 ) demonstrated the presence of microorganisms in air.
- He disproved the concept of spontaneous generation through controlled experiments.
- In 1873, Pasteur proposed the germ theory of disease, linking microbes to disease causation.
Contributions of Robert Koch
- Robert Koch ( 1843–1910 ) provided experimental proof of germ theory.
- In 1877, he demonstrated that anthrax is caused by a specific bacterium.
- His work established a direct relationship between specific microbes and specific diseases.
Golden Age of Bacteriology
- The late 19th century marked rapid discoveries of disease-causing organisms:
- Gonococcus (1879)
- Typhoid bacillus and pneumococcus (1880)
- Tubercle bacillus (1882)
- Cholera vibrio (1883)
- Diphtheria bacillus(1884)
- This period is known as the “golden age of bacteriology”.
Impact on Medical Science
- Germ theory replaced earlier speculative explanations of disease.
- It established the concept of specific aetiology, where each disease has a specific cause.
- Medicine shifted from dogma and superstition to evidence-based scientific practice.
Significance
- The germ theory provided the foundation for modern microbiology, immunology, and public health.
- It enabled development of preventive measures, including sanitation, vaccination, and infection control.
Birth of preventive medicine
- Preventive medicine originated in the 18th century as a discipline distinct from public health.
- It developed even before the identification of specific causative agents of diseases.
- James Lind ( 1716–1794 ) demonstrated in 1753 that intake of fresh fruits and vegetables prevents scurvy.
- Edward Jenner ( 1749–1823 ) introduced vaccination against smallpox in 1796.
- These discoveries marked the beginning of specific disease prevention strategies.
Foundation After Germ Theory
- Preventive medicine gained a scientific basis after the germ theory of disease was established.
- The late 19th century witnessed major advances:
- Anti-rabies treatment by Louis Pasteur (1883)
- Cholera vaccine (1892)
- Diphtheria antitoxin (1894)
- Anti-typhoid vaccine (1898)
- Development of antiseptics and disinfectants (1827–1912)
Discovery of Disease Transmission
- Understanding modes of transmission enabled targeted prevention:
- David Bruce (1896) showed African sleeping sickness is transmitted by the tsetse fly.
- Ronald Ross (1898) demonstrated malaria transmission by the Anopheles mosquito.
- Walter Reed (1900) established yellow fever transmission by the Aedes mosquito.
Control Measures and Public Health Actions
- Knowledge from bacteriology enabled specific control measures, including:
- Quarantine
- Water purification
- Pasteurization of milk
- Food protection
- Proper sewage disposal
- Vector control(destruction of insects)
- Disinfection practices
Advances in Diagnosis
- Development of laboratory methods allowed early detection of diseases, improving prevention and control.
Early Scope and Limitations
- Initially, preventive medicine focused mainly on control of infectious diseases.
- Modern concepts such as primary, secondary, and tertiary prevention were not yet developed.
Significance
- Preventive medicine laid the foundation for modern disease control strategies.
- It emphasized anticipation, interruption of transmission, and early detection as key principles of healthcare.
MODERN MEDICINE
- By the end of the 19th century, medicine was clearly divided into two main branches: curative medicine and preventive (public health) medicine.
- After 1900, medicine progressed rapidly towards specialization and adopted a more scientific and evidence-based approach to disease.
- The pattern of diseases gradually shifted. Acute infectious diseases declined due to improved control measures.
- Consequently, non-communicable diseases such as cancer, diabetes, cardiovascular diseases, mental disorders, and accidents became leading causes of mortality, especially in industrialized regions.
- These conditions could not be fully explained by the germ theory of disease, nor effectively managed by single-target treatments (“magic bullets”).
- It became evident that disease causation involves multiple determinants, including social, economic, genetic, environmental, and psychological factors.
- Many of these determinants are strongly associated with lifestyle and behavioural patterns.
- The traditional germ theory gradually evolved into the concept of multifactorial causation of disease.
- The idea was initially proposed during 1819–1901, but it gained recognition later with advancements in epidemiology.
- Epidemiologists played a crucial role in identifying risk factors, improving understanding of disease causation, and shaping modern preventive strategies.
- Modern medicine is therefore characterized by an integrated approach that combines clinical care, prevention, and risk-factor analysis.
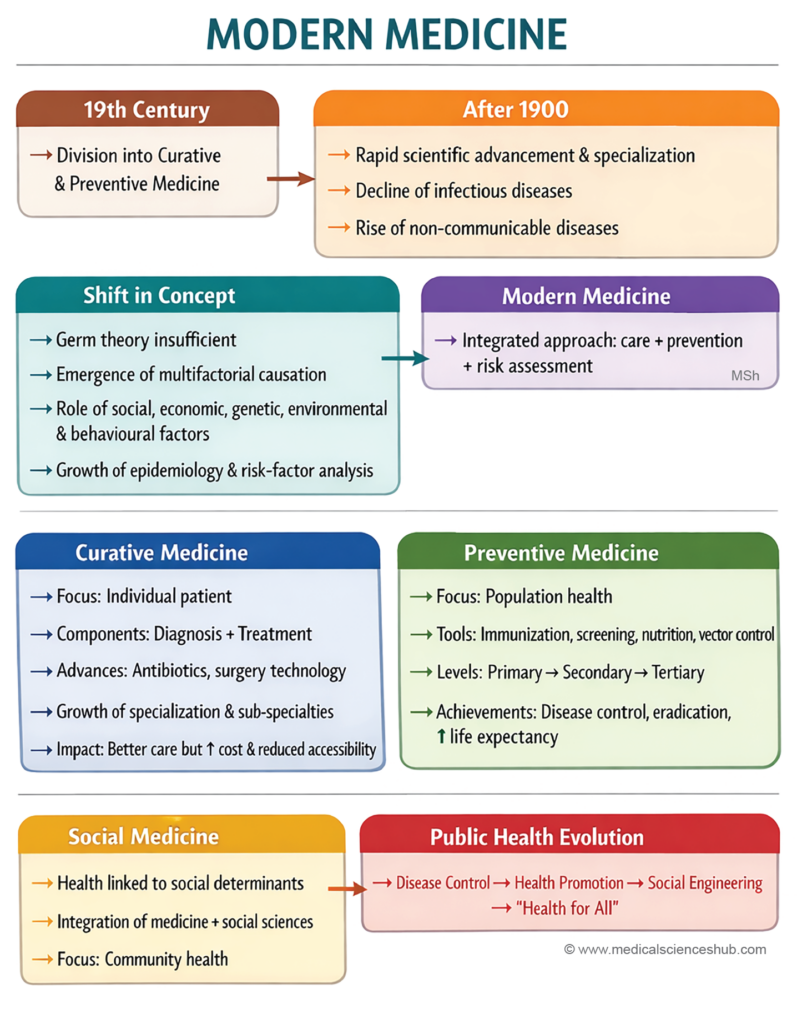
1. Curative Medicine
- Curative medicine has existed for thousands of years, but modern clinical medicine in its present scientific form is only about 100 years old.
- The primary aim of curative medicine is the elimination of disease in an individual patient, rather than addressing disease at the population level.
- It relies on two major components: diagnosis and treatment.
- Over time, diagnostic methods have become highly refined, precise, and technologically advanced, improving early detection and accuracy.
- The therapeutic armamentarium has expanded to include more specific and potent interventions, including drugs, surgical procedures, and supportive care technologies.
Advances in Therapeutics
- A major transformation occurred during the mid-20th century with the introduction of antibacterial agents and antibiotics.
- These agents significantly improved the management of infectious diseases and reduced mortality rates.
- The concept of allopathic treatment involves the use of therapeutic agents that counteract or neutralize disease processes.
Current Scope
- Curative medicine now encompasses a vast and organized system of scientific knowledge, clinical skills, pharmaceuticals, and medical technologies.
- It not only focuses on treating diseases but also aims at preserving life and improving patient outcomes.
- Continuous advancements have strengthened its role in managing both acute and chronic conditions effectively.
Growth of Specialization in Modern Medicine
- Over the past 100 years, medicine has undergone rapid expansion in specialization, driven by advances in medical technology.
- Changes in the pattern and distribution of diseases and evolving societal focus on age and sex groups have contributed to this trend.
Types of Specialties
- Some specialties are based on specific skills, such as surgery, radiology, and anaesthesia.
- Others are organized according to body systems or organs, including ENT, ophthalmology, cardiology, and gynaecology.
- Certain specialties focus on age or sex groups, such as paediatrics, geriatrics, and obstetrics.
Emergence of Sub-specialties
- Each major specialty has further divided into sub-specialties with advanced expertise.
- For example, paediatrics includes neonatology, perinatology, paediatric cardiology, paediatric neurology, and paediatric surgery.
- This trend has led to increasing micro-specialization, raising questions about its necessity and efficiency.
Impact of Specialization
- Specialization has significantly improved the quality and precision of medical care.
- However, it has also increased the cost of healthcare, making specialized services less accessible to the average population without financial support.
- This imbalance challenges the principle of equitable healthcare distribution and may require social or policy-level interventions.
- It has also contributed to the decline of general practice and the relative isolation of primary care physicians within the healthcare system.
2. Preventive Medicine
- Preventive medicine emerged as a distinct branch separate from public health, with a focus on healthy populations.
- It is applied at the community or population level, rather than to individual patients.
- The primary goals are prevention of disease and promotion of health through organized interventions.
Early Achievements
- Major successes occurred in the early 20th century with the development of bacterial vaccines and antisera.
- These interventions significantly reduced morbidity and mortality from diseases such as diphtheria, tetanus, and typhoid fever.
- Immunization programs became a key strategy in controlling infectious diseases.
Advances in Viral Vaccines
- Progress in tissue culture techniques enabled the development of viral vaccines.
- Important milestones include the introduction of polio vaccines in 1955 and 1960.
- These advances strengthened large-scale immunization efforts worldwide.
Major Public Health Success
- The global eradication of smallpox represents a landmark achievement.
- The last reported case occurred in 1977 in Somalia, confirming successful elimination.
Ongoing Developments
- Research continues to develop new and improved vaccines against diseases such as malaria, leprosy, syphilis, parasitic infections, and certain cancers.
- Preventive medicine increasingly integrates epidemiology, immunology, and health education to enhance disease control strategies.
Expansion of Preventive Medicine
- Preventive medicine extends beyond vaccination and quarantine to include multiple health protection strategies.
- Advances in nutrition science have added an important dimension to disease prevention.
- Identification of deficiencies in vitamins, minerals, proteins, and dietary fibre has improved understanding of health maintenance.
- Targeted interventions have been developed to prevent nutritional blindness (vitamin A deficiency) and iodine deficiency disorders.
Role of Chemical Control
- The discovery of synthetic insecticides such as DDT, HCH, and malathion transformed vector control strategies.
- These agents significantly reduced transmission of vector-borne diseases like malaria, leishmaniasis, plague, and rickettsial infections.
- Despite challenges such as insecticide resistance and environmental concerns, these chemicals remain important in disease control.
- The Bhopal disaster (India, 1984) highlighted the risks associated with improper handling of industrial chemicals.
Chemotherapy and Chemoprophylaxis
- The introduction of sulpha drugs, antimalarials, antibiotics, anti-tubercular, and anti-leprosy drugs strengthened preventive strategies.
- Chemoprophylaxis and mass drug administration are now widely used to prevent and control diseases at the community level.
Impact on Disease Pattern
- Improved prevention and treatment of infectious diseases have altered the epidemiological pattern in populations.
- There has been a decline in infectious disease burden and an increase in life expectancy, especially in developing countries.
- Preventive medicine now integrates nutrition, vector control, and pharmacological interventions to achieve comprehensive disease control.
Disease Eradication and New Strategies
- A new concept, disease eradication, emerged during the 20th century as a major goal of preventive medicine.
- This concept was successfully applied in the eradication of smallpox, with the last case reported in 1977.
- Efforts are ongoing for eradication or elimination of diseases such as measles, tetanus, guinea worm disease, and endemic goitre.
Development of Screening
- The concept of screening was developed for detecting disease in the presymptomatic stage.
- In the 1930s, commonly used screening tests included the serological test for syphilis and chest X-ray for tuberculosis.
- By the early 1950s, screening evolved into multiphase screening, enabling detection of multiple conditions simultaneously.
- Despite debates regarding its effectiveness, screening remains essential in early diagnosis among apparently healthy individuals.
Risk-Factor Identification
- Screening expanded to include detection of risk factors and identification of high-risk groups.
- This approach is particularly important for chronic diseases, where specific curative measures are limited.
- Regular health check-ups aid in early detection of cancer, diabetes, rheumatic diseases, and cardiovascular disorders, often termed “diseases of civilization.”
Population and Reproductive Health
- Preventive medicine now addresses challenges related to population growth, especially in developing countries.
- Rapid population increase contributes to social, economic, environmental, and political issues.
- Strategies include advancement in contraceptive technology and research in human fertility regulation.
- Genetic counselling has gained importance in preventing hereditary disorders and improving population health outcomes.
Current Scope of Preventive Medicine
- Preventive medicine has become a rapidly expanding field in modern healthcare.
- Progress in curative treatment has not reduced the importance of prevention; both approaches are complementary.
- Preventive strategies are now applied to chronic, degenerative, hereditary diseases, and conditions related to ageing.
- Emerging areas such as preventive paediatrics, preventive cardiology, and geriatrics reflect this expanding scope.
Determinants and New Opportunities
- Advances in scientific knowledge, improved living standards, and better health education have created new opportunities for disease prevention.
- Preventive medicine increasingly addresses broader determinants including environmental, social, and economic factors.
Levels of Prevention
- Three standard levels of prevention are recognized:
- Primary prevention aims to prevent disease in healthy individuals through measures such as immunization and health education.
- Secondary prevention focuses on early detection and prompt treatment in individuals with existing disease.
- Tertiary prevention aims to limit disability and promote rehabilitation in chronic conditions.
Concept and Approach
- Modern preventive medicine is defined as the science and practice of health promotion, disease prevention, disability limitation, and rehabilitation.
- It involves a more individual-centered approach compared to traditional public health practices.
- Preventive medicine functions as anticipatory medicine, emphasizing early action before disease progression.
3. Social Medicine
- Social medicine developed mainly as a European discipline, emphasizing the relationship between society and health.
- The idea that medicine is a social science emerged in the late 19th century.
- Early contributions in 1847 and 1848 highlighted the influence of social conditions on disease, but these ideas were not widely accepted at that time.
- The rise of the germ theory of disease and advances in microbiology temporarily limited the growth of social perspectives in medicine.
Revival and Conceptual Development
- In 1911, the concept of social medicine was revived, stressing the role of social determinants in disease causation.
- The term “social pathology” was introduced to describe the impact of social factors on health.
- Alternative terms such as geographical pathology and population pathology were also used.
- In 1912, the Belgian Social Medicine Association was established, marking institutional development in this field.
Influence of Social Sciences
- Progress in disciplines such as sociology, psychology, and anthropology strengthened the understanding of health and disease.
- It was recognized that humans are both biological and social beings, and disease has social causes, consequences, and interventions.
Expansion and Institutionalization
- The concept of social medicine spread to other countries, particularly England.
- It was promoted as an evolution of medical practice, integrating clinical and social perspectives.
- A Chair of Social Medicine was established at Oxford in 1942, followed by similar academic developments in other universities.
- Social medicine contributed to a broader understanding of health inequalities, living conditions, and community-based care.
Concept and Scope of Social Medicine
- Social medicine refers to the study of humans as social beings within their total environment.
- Its primary focus is the health of communities, rather than only individual patients.
- It is based on the integration of medicine and sociology, highlighting their interdependence.
- The discipline reflects a holistic approach, considering biological, social, and environmental determinants of health.
Interpretations of Social Medicine
- Social medicine has both broad and narrow meanings in contemporary usage.
- In the broad sense, it represents a humanitarian approach and may include patient care, disease prevention, and health service organization.
- In the restricted sense, it is closely linked to epidemiology and the study of health needs and medical care of populations.
Core Orientation
- Social medicine is not a completely new branch but a reorientation of medicine to meet evolving societal needs.
- It emphasizes the strong relationship between health and social factors, including living conditions and socioeconomic status.
- The discipline relies heavily on epidemiological methods to investigate disease patterns and causes.
Interdisciplinary Contributions
- It has developed strong links with social sciences and statistics, improving the analysis of disease distribution and determinants.
- These collaborations help in understanding the social aetiology of diseases and planning appropriate interventions.
Limitations and Criticism
- Social medicine has been criticized for being largely academic in orientation.
- It has often remained detached from practical healthcare services, with greater emphasis on research in health systems and chronic diseases.
- Despite these limitations, it has significantly contributed to the expansion of modern medical concepts.
Changing Concepts in Public Health
- The evolution of public health can be divided into four distinct phases, reflecting changes in knowledge and practice over time.
a. Disease Control Phase (1880–1920)
- During the late 19th century, public health focused mainly on sanitary reforms and legislation.
- Interventions targeted the physical environment, including improvement of water supply, sewage disposal, waste management, and housing conditions.
- These measures were not directed at specific diseases due to limited scientific and microbiological knowledge at that time.
- Despite this limitation, environmental interventions led to a significant reduction in disease incidence and mortality rates.
- The approach emphasized population-level interventions rather than individual medical care.
- This phase laid the foundation for later developments in disease-specific prevention and control strategies.
b. Health Promotional Phase (1920–1960)
- During the period 1920–1960, the concept of health promotion became an important component of public health.
- It was recognized that earlier public health efforts had overlooked the individual, focusing mainly on environmental control.
- The State’s responsibility for ensuring the health of individuals was increasingly emphasized.
- Public health expanded beyond disease control to include promotion of positive health and well-being.
Expansion of Services
- A range of personal health services was introduced to support individual health:
- Maternal and child health (MCH) services
- School health services
- Industrial (occupational) health services
- Mental health services
- Rehabilitation services
- The development of public health nursing was a direct outcome of this expanded approach.
- Public health departments began to broaden their programs to include preventive and promotive care.
Conceptual Foundation
- In 1920, a comprehensive definition of public health was proposed, emphasizing three core functions:
- Prevention of disease
- Prolongation of life
- Promotion of health and efficiency through organized community efforts
- This definition continues to represent the fundamental philosophy of public health in modern practice.
State Responsibility and Health Service Development
- With the State assuming direct responsibility for individual health, major initiatives for human development were launched during the first half of the 20th century.
a. Basic Health Services and Health Centres
- The concept of basic health services was implemented through Primary Health Centres (PHCs) and subcentres in both rural and urban areas.
- The development of health centres marked a significant milestone in public health organization.
- The idea of a health centre was first proposed in 1920 in England.
- In 1931, the League of Nations Health Organization recommended the establishment of such centres globally.
- In India, the Bhore Committee (1946) strongly advocated health centres to deliver integrated curative and preventive services.
- Many developing countries prioritized PHCs as a foundation for accessible and equitable healthcare delivery.
b. Community Development Programme
- Another key initiative was the Community Development Programme, aimed at rural development through community participation.
- It emphasized local initiative, self-reliance, and collective action in improving living conditions.
- However, the programme faced limitations due to overambitious goals and insufficient resources, leading to its decline.
Impact
- Despite setbacks in community development efforts, the establishment of PHCs and subcentres created essential health infrastructure, particularly in rural areas.
- These developments strengthened the delivery of basic health services and improved access to care at the community level.
c. Social Engineering Phase (1960–1980)
- During 1960–1980, public health entered the “social engineering” phase due to changing disease patterns.
- Advances in preventive medicine led to effective control of many acute infectious diseases in developed countries.
- As a result, chronic non-communicable diseases such as cancer, diabetes, cardiovascular diseases, alcoholism, and drug addiction became more prominent, especially in affluent societies.
Emergence of New Concepts
- Traditional public health measures like isolation, immunization, and disinfection were insufficient to address these conditions.
- These diseases could not be explained solely by the germ theory of disease.
- The concept of risk factors emerged to explain their multifactorial causation, including lifestyle and behavioural determinants.
Shift in Public Health Approach
- Chronic diseases imposed a long-term burden on individuals and society, unlike the rapid mortality seen in infectious diseases.
- Public health strategies shifted towards social and behavioural interventions.
- Greater emphasis was placed on prevention, health promotion, and rehabilitation of chronic conditions.
Integration with Preventive Medicine
- During this phase, the goals of public health and preventive medicine became closely aligned:
- Prevention of disease
- Promotion of health
- Prolongation of life
Concept of Community Health
- The traditional meaning of public health expanded and evolved.
- The term “community health” gained preference, reflecting a broader focus on population-based services and holistic care.
- Community health integrates preventive, promotive, and rehabilitative services for the entire population.
d. “Health for All” Phase (1981–2000 A.D.)
- During 1981–2000, global attention focused on health inequalities between developed and developing countries.
- Despite medical advances, a large proportion of populations in developing regions lacked access to basic health determinants such as nutrition, sanitation, safe water, education, and healthcare.
- Only about 10–20% of people in developing countries had adequate access to health services.
- Infant mortality rates ranged from 60 to 250 per 1000 live births, and life expectancy was approximately 30% lower compared to developed nations.
Recognition of Global Inequity
- A significant proportion of the global population had little or no access to healthcare services.
- Even where services existed, they were often inadequate or inappropriate for local health needs.
- These disparities highlighted the urgent need for equitable distribution of healthcare resources.
Global Response and Strategy
- There was growing international consensus that health is a fundamental human right.
- Efforts were directed toward reducing the health gap between rich and poor populations, both within and between countries.
- Emphasis was placed on providing primary health care, especially for maternal and child health and control of common infectious diseases.
“Health for All” Initiative
- In 1981, member states of the World Health Organization (WHO) adopted the goal of “Health for All by the year 2000”.
- The objective was to achieve a level of health that enables individuals to lead socially and economically productive lives.
- This strategy required coordinated efforts from public health systems, medical sciences, and other sectors such as education, nutrition, and sanitation.
Significance
- The “Health for All” approach emphasized equity, accessibility, and community participation in healthcare delivery.
- It marked a shift towards comprehensive primary health care as the cornerstone of global health policy.
MEDICAL REVOLUTION
State of the Art
- Modern medicine has progressed from studying the whole organism to focusing on organs, cells, and molecular mechanisms.
- This transition reflects advances in cell biology, biochemistry, and molecular genetics.
- Major discoveries include the biological role of nucleic acids and the genetic code, which regulate vital life processes.
Advances in Medical Science
- Medicine has developed a vast and highly technical knowledge base, supported by sophisticated technologies.
- New capabilities allow direct intervention in human biological processes, improving diagnosis, treatment, and prevention.
- Important developments include:
- Genetic counselling and genetic engineering
- Prenatal diagnosis of sex and genetic disorders
- In vitro fertilization (IVF)
- Advances in organ transplantation
- Use of artificial organs, such as dialysis (artificial kidney) and artificial heart devices
- Emerging techniques like cloning (asexual reproduction of genetically identical individuals)
- Specialized procedures such as psychosurgery
Implications of the Medical Revolution
- These advancements enable greater control over human biology and disease processes.
- Medicine now aims not only to treat illness but also to preserve and enhance life.
- The field has entered a new evolutionary stage, characterized by rapid innovation and expanding possibilities.
- Continued progress is expected to further improve health outcomes and quality of life, while also raising ethical and social considerations.
Social Control of Medicine
- In 1849, it was emphasized that medicine is closely linked with social and political systems, anticipating later developments in health policy.
- With scientific progress, medicine became increasingly specialized, institutionalized, and technology-driven.
- This transformation led to concerns that medical services were not equitably distributed across populations.
Inequality in Medical Care
- Rising costs of healthcare resulted in two parallel systems:
- One catering to the wealthy population
- Another limited system available to the economically disadvantaged
- Charitable and voluntary organizations attempted to reduce this gap by providing free or subsidized care.
- A broader view emerged that access to modern medicine should be a universal right, not dependent on financial status.
Concept of Socialization of Medicine
- The idea of “socialization of medicine” developed as a response to inequalities in healthcare access.
- It aimed to ensure that medical services are available to all individuals, regardless of socioeconomic status.
Distinction Between Related Concepts
- Social medicine focuses on the social determinants of health and community well-being.
- State medicine refers to the provision of free medical services funded and delivered by the government.
- Socialized medicine involves state-supported healthcare and medical education, but services are organized and regulated by professional bodies rather than directly controlled by the government.
Overall Significance
- Social control of medicine emphasizes the need for equity, accessibility, and organized healthcare systems.
- It reflects the growing recognition that healthcare is a social responsibility requiring coordinated efforts between the state, professionals, and society.
Evolution of Socialized Health Systems
- Germany (1883) introduced compulsory sickness insurance, marking the beginning of organized social health protection.
- This model influenced other countries: England (1911) and France (1928) adopted similar insurance systems.
- Great Britain (1946) established a nationalized health service, ensuring wider access to care.
- Several nations, including socialist countries in Europe, New Zealand, and Cuba, implemented systems to socialize health services.
- Russia (USSR) was the first to fully socialize medicine, granting citizens a constitutional right to healthcare.
- Medicine gradually shifted from private practice to a social institution within broader welfare systems.
Advantages of Socialization
- Socialization promotes equity in healthcare access and reduces disparities between socioeconomic groups.
- It minimizes competition among physicians for patients, encouraging organized service delivery.
- Healthcare services become universally accessible, often free at the point of use, funded by the State.
Limitations and System Variations
- Different countries adopted varying degrees of social control, resulting in diverse health system models.
- Each system has its own advantages and limitations, depending on governance and resource allocation.
- Socialization alone does not guarantee effective utilization of health services.
Role of Community Participation
- Greater emphasis is now placed on community participation in healthcare.
- It involves individuals and families taking responsibility for their own health and that of the community.
- Communities actively engage in planning, organization, and management of health services.
- This approach is often described as “Health by the People”, promoting self-reliance and sustainability.
Overall Perspective
- Modern healthcare systems combine state support, professional organization, and community involvement.
- The integration of these elements helps achieve accessible, equitable, and effective healthcare delivery.
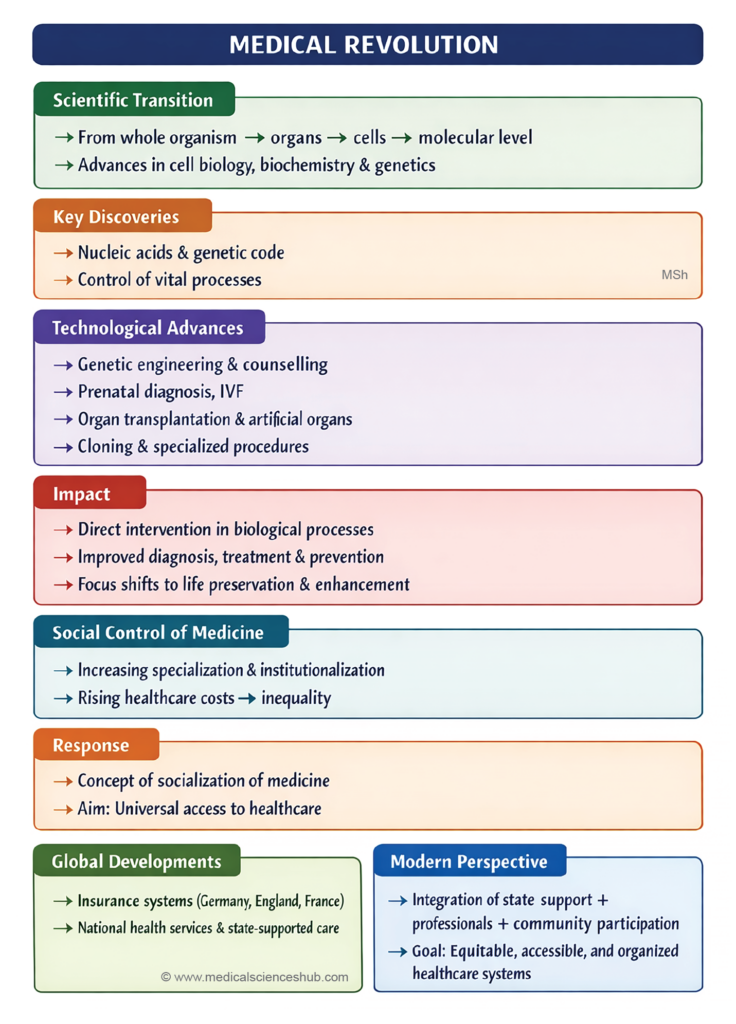
Family and Community Medicine
Historical Background
- In 1923, Dr. Francis Peabody highlighted that increasing specialization had fragmented healthcare delivery.
- He advocated a return to the general physician (family physician) who provides comprehensive and continuous care.
- In 1966, the Millis Commission Report and Willard Committee Report in the United States reinforced the need for broad-based primary care.
- In 1971, the American Academy of General Practice (established in 1947) was renamed the American Academy of Family Physicians, emphasizing family-oriented healthcare and academic recognition of the specialty.
Concept and Scope
- Family and community medicine emerged as a response to excessive medical specialization.
- This field focuses on holistic care, addressing the biological, social, and environmental aspects of health.
- Unlike other specialties, it is not based on a specific organ or disease, but on social units such as the family and the community.
Core Features
- It provides comprehensive, continuous, and coordinated care for individuals and families.
- Emphasis is placed on primary care, prevention, and health promotion.
- It integrates clinical medicine with public health principles.
Relationship Between Family and Community Medicine
- Family medicine focuses on the individual and family unit, ensuring personalized care.
- Community medicine addresses the health needs of populations and public health systems.
- Both disciplines are interrelated and mutually reinforcing, contributing to integrated healthcare delivery.
Overall Significance
- Family and community medicine act as a counterbalance to over-specialization in modern medicine.
- They promote accessible, equitable, and patient-centered healthcare, strengthening the overall health system.
Family Medicine
Concept and Orientation
- Family medicine represents a renewed focus on the human, social, and cultural dimensions of health and disease.
- It recognizes the family as the central unit of healthcare, where prevention and care can be effectively integrated.
- The discipline emphasizes a holistic approach, combining preventive, promotive, curative, and rehabilitative services.
Definition and Scope
- Family medicine is a medical specialty that is not limited to a specific organ or disease.
- It is family-oriented, providing care across all ages, sexes, and disease conditions.
- Care begins at the first point of contact and continues through the management of chronic conditions and rehabilitation.
Family Practice
- When applied in clinical settings, family medicine is practiced as family practice.
- It provides continuous and comprehensive care to individuals and their families over time.
- Family practice is described as a horizontal specialty, sharing knowledge and functions with multiple clinical disciplines such as paediatrics and internal medicine.
Role in Primary Care
- Family medicine is specifically designed to deliver primary health care services.
- It ensures accessible, coordinated, and patient-centered care at the community level.
- The approach strengthens the link between clinical care and public health, improving overall health outcomes.
Significance
- Family medicine supports early diagnosis, continuity of care, and long-term health management.
- It plays a key role in achieving comprehensive and equitable healthcare delivery systems.
Community Medicine
Concept and Evolution
- Community medicine is a relatively recent discipline in modern healthcare.
- It evolved from earlier fields such as public health, preventive medicine, and social medicine.
- All these disciplines share a common objective: prevention of disease and promotion of health.
Definition and Scope
- Community medicine focuses on the health of populations rather than individuals.
- It involves assessing the health needs of both healthy and diseased individuals within a community.
- The discipline includes:
- Measurement of community health needs
- Planning and administration of health services
- Research and teaching in population health
Variability in Definition
- There is no single universally accepted definition of community medicine.
- Multiple definitions exist, reflecting differences in health systems and professional perspectives.
- International guidance suggests that each country should define community medicine based on its geography, resources, and health priorities.
Functions and Responsibilities
- Community medicine specialists are involved in health planning, service delivery, and evaluation.
- They apply epidemiological and statistical methods to understand disease patterns.
- The discipline integrates clinical knowledge with public health principles for effective healthcare delivery.
Challenges and Issues
- The emergence of community medicine has created confusion regarding roles and professional identity.
- Differences exist between academic and service-oriented functions.
- Despite these challenges, community medicine plays a crucial role in population-based healthcare systems.
HEALTH CARE REVOLUTION
- It was increasingly recognized that existing health services were inadequate in both developed and developing countries.
- Health services often failed to meet the expected standards of care for the population.
Limitations of Health Services
- Services did not provide universal coverage, leaving large sections of the population underserved.
- There was unequal distribution of resources, with shortages in some regions and duplication of services in others.
- A significant proportion of people in developing countries, especially in rural areas, lacked access to basic healthcare.
- Health services tended to favor urban populations and economically privileged groups.
Inequality and Health Disparities
- Despite recognition of health as a fundamental human right, many individuals remained deprived of essential care.
- A vicious cycle of poverty and ill health persisted, particularly in low-resource settings.
- There were marked differences in health status between countries and among population groups within the same country.
Economic Concerns
- The cost of healthcare continued to rise without a corresponding improvement in quality and outcomes.
- This imbalance contributed to inefficiencies and reduced accessibility.
Need for Reform
- Growing dissatisfaction with existing systems led to a demand for equitable, accessible, and efficient healthcare services.
- These concerns laid the foundation for a health care revolution, emphasizing universal access and improved service delivery.
Health for All
New Approaches in Health Care
- Emerging ideas emphasized social justice and equity as essential principles in healthcare delivery.
- Greater importance was given to community participation in planning and implementing health services.
- The concept of health expanded to include its link with overall development, including social and economic progress.
- Recognition of the need for strong political commitment became crucial for effective health system reforms.
- These developments called for innovative and comprehensive approaches to improve healthcare outcomes.
Global Policy Milestone (1977)
- In May 1977, the 30th World Health Assembly set a major global health objective.
- It declared that the primary social goal was achieving a level of health enabling people to lead socially and economically productive lives.
- This resolution led to the global strategy of “Health for All by the year 2000.”
Concept of “Health for All”
- In the long-term perspective, it aims at achieving the highest possible level of health for all populations.
- In the short-term perspective, it ensures that all individuals attain a minimum acceptable level of health.
- This minimum level enables people to work productively and participate actively in community life.
- The “Health for All” goal reflects a shift towards universal access, equity, and community-based care.
- It integrates health, development, and social welfare into a unified framework.
- The approach emphasizes that health improvement requires multi-sectoral collaboration and sustained policy efforts.
Meaning and Scope of “Health for All”
- Health for All implies that essential health services are accessible to every individual within a community.
- It requires the removal of barriers to health, including:
- Malnutrition
- Lack of education (ignorance)
- Communicable and non-communicable diseases
- Unsafe water supply
- Poor housing and sanitation
- The achievement of this goal depends on continuous progress in medicine and public health systems.
Holistic and Intersectoral Approach
- Health for All is a comprehensive concept, extending beyond the medical field.
- It requires coordinated efforts across multiple sectors, including:
- Agriculture (nutrition and food security)
- Industry (safe working conditions)
- Education (health awareness)
- Housing and sanitation
- Communication systems (health information dissemination)
- This reflects a multisectoral approach to health improvement.
Global Commitment and Target
- The goal of achieving Health for All by 2000 A.D. was adopted as a central objective of WHO and its member states.
- It symbolized a global commitment to ensure a minimum acceptable level of health for all populations.
Significance
- Health for All represents a transformative and equity-based approach to healthcare.
- It emphasizes universal access, prevention, and social development.
- The concept highlights that health improvement requires collective action across sectors and sustained policy efforts.
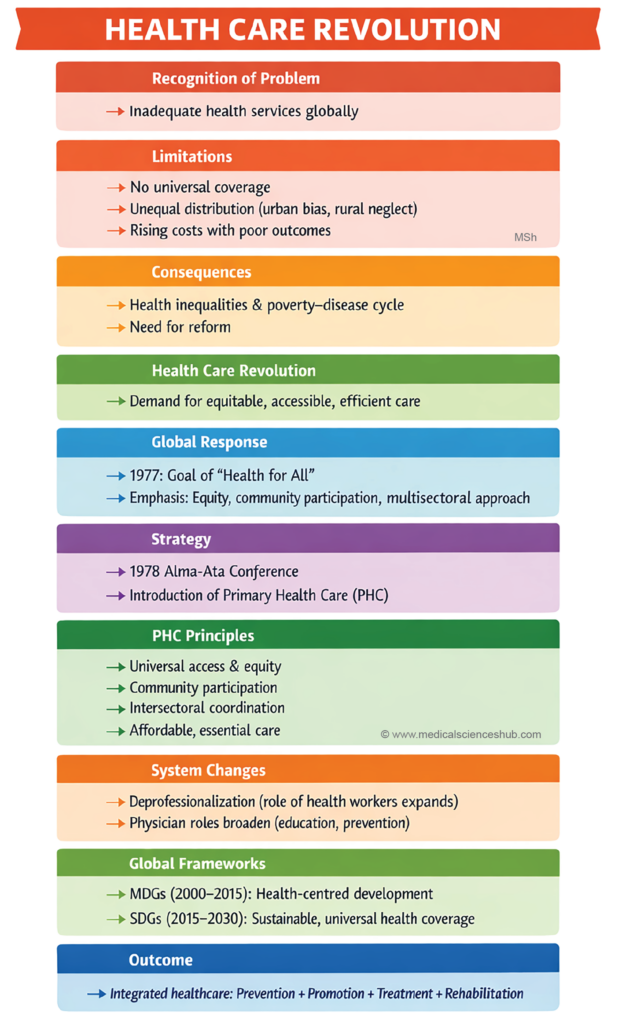
Primary Health Care (PHC)
- Recognition of the failure of existing health systems led to the search for alternative approaches to healthcare delivery.
- At the WHO–UNICEF International Conference (Alma-Ata, USSR, 1978), representatives from 134 countries and several voluntary agencies participated.
- The conference declared that global health inequalities between and within countries were socially, politically, and economically unacceptable.
- It endorsed the goal of “Health for All by 2000 A.D.” and identified Primary Health Care (PHC) as the key strategy to achieve it.
Concept of Primary Health Care
- PHC is a comprehensive approach that integrates all essential factors influencing health at the community level.
- It includes at least eight essential elements of healthcare, collectively termed “essential health care.”
- Services are designed to be scientifically sound, socially acceptable, and economically feasible.
- PHC services are:
- Accessible to all individuals at the first level of contact
- Affordable and efficient in terms of cost and organization
- Focused on improving the living conditions of individuals, families, and communities
Core Principles
- PHC is based on the following principles:
- Equity in distribution of health services
- Universal coverage and accessibility
- Community participation in planning and implementation
- Intersectoral coordination across different development sectors
Significance
- PHC represents a major shift from conventional healthcare systems, which were often hospital-centered and urban-focused.
- It integrates promotive, preventive, curative, and rehabilitative services at the community level.
- PHC is closely linked with socio-economic development, emphasizing that health improvement requires broader developmental efforts.
Alma-Ata Declaration and National Action
- The Alma-Ata Declaration (1978) urged all governments to develop national policies, strategies, and action plans for implementing Primary Health Care (PHC).
- PHC was to be integrated as a core component of national health systems.
- Each country was encouraged to adapt PHC according to its own resources, needs, and socio-economic conditions.
Global Strategy Development
- In 1981, the 34th World Health Assembly adopted the Global Strategy for Health for All.
- This strategy provided a framework for countries to achieve the goal of “Health for All by 2000 A.D.”.
Early Implementation and Progress
- Many countries initiated PHC programmes with the central theme of universal access to essential health services.
- Early implementation demonstrated the feasibility of delivering basic, community-based healthcare.
Challenges and Significance
- The goal of Health for All by 2000 A.D. posed a complex and demanding challenge due to wide disparities in health systems.
- It required strong political commitment, resource allocation, and intersectoral coordination.
- The Alma-Ata Declaration served as a guiding framework, emphasizing equity, accessibility, and community participation.
- PHC implementation marked a turning point in global health policy, shifting focus toward community-oriented and equitable healthcare systems.
- It reinforced the principle that achieving health goals requires sustained national and international efforts.
Deprofessionalization of Medicine
- The implementation of Primary Health Care (PHC) has led to partial deprofessionalization of medicine.
- This concept involves sharing healthcare responsibilities with trained non-physician personnel.
- It aims to improve accessibility and coverage of health services, especially in underserved areas.
Role of Non-Professional Health Workers
- A new cadre of health workers with limited formal training has become essential in service delivery.
- These include:
- Community health workers
- Anganwadi workers
- Multipurpose health workers
- Practitioners of indigenous medicine
- Social workers
- These personnel function as part of integrated health teams, extending care to the community level.
Changing Role of the Physician
- The role of the physician has expanded beyond traditional clinical functions.
- In addition to diagnosis and treatment, physicians now act as:
- Health educators
- Case-finders (early detection of disease)
- Preventive care providers
- Counsellors
- Agents of social change
Significance
- Deprofessionalization enhances community participation and promotes cost-effective healthcare delivery.
- It allows wider coverage of essential services without relying solely on highly specialized professionals.
- This approach strengthens the primary healthcare system and supports the goal of universal health access.
Millennium Development Goals (MDGs)
- In September 2000, representatives from 189 countries met at the Millennium Summit in New York.
- They adopted the United Nations Millennium Declaration, outlining global commitments.
- Key areas included:
- Peace, security, and disarmament
- Development and poverty eradication
- Environmental protection
- Human rights and good governance
- Protection of vulnerable populations
- Special focus on Africa
- Strengthening the United Nations
- A Road Map was created with specific goals and targets to be achieved by 2015.
Core Focus of MDGs
- The goals related to development and poverty reduction are collectively known as the Millennium Development Goals (MDGs).
- The MDGs placed health at the centre of global development efforts.
Health and Development Link
- The MDGs aimed to reduce:
- Poverty and hunger
- Disease burden
- Gender inequality
- Lack of education
- Limited access to safe water
- Environmental degradation
- Health improvement was recognized as both a goal and a determinant of development.
Health-Related Goals and Indicators
- Out of the 8 MDGs, 3 goals are directly related to health.
- Additionally:
- 8 of the 18 targets are health-related
- 18 of the 48 indicators measure health outcomes
- The remaining goals have indirect but significant effects on health status.
Significance
- The MDGs represent a global commitment to improve health, equity, and living conditions.
- They emphasize integrated, multi-sectoral strategies to address determinants of health.
- The framework guided international efforts to achieve measurable improvements in population health by 2015.
Sustainable Development Goals (SDGs)
- In September 2015, the United Nations General Assembly adopted the 2030 Agenda for Sustainable Development.
- The agenda consists of 17 Sustainable Development Goals (SDGs) to be achieved by 2030.
- It integrates three core dimensions: economic development, social progress, and environmental protection.
- The framework is structured around five key themes: people, planet, prosperity, peace, and partnership.
Link Between Development and Health
- The SDGs emphasize that poverty eradication, reduction of inequalities, economic growth, and environmental sustainability are interconnected.
- These determinants are closely related to population health and well-being.
- Health is both a central outcome and a driving factor in sustainable development.
Health Goal: SDG 3
- SDG 3 focuses on ensuring healthy lives and promoting well-being for all at all ages.
- It is a comprehensive health goal with linkages to multiple other SDGs.
Targets Under SDG 3
- SDG 3 includes 13 targets addressing major health priorities:
- 4 targets related to the unfinished and expanded Millennium Development Goals (MDGs)
- 4 targets addressing non-communicable diseases, mental health, injuries, and environmental health risks
- 4 targets focusing on implementation strategies, including health system strengthening
- A central component is achieving Universal Health Coverage (UHC).
Importance of Universal Health Coverage
- UHC ensures access to essential health services without financial hardship.
- It is critical for achieving all other health-related targets and strengthening resilient health systems.
- Implementation requires an integrated and coordinated health service delivery system, minimizing fragmentation.
Overall Significance
- The SDGs provide a comprehensive global framework linking health with development.
- They promote equity, sustainability, and multisectoral collaboration.
- The agenda aims to achieve long-term improvements in health status and quality of life worldwide.
Conclusion
- Contemporary medicine is no longer limited to the diagnosis and treatment of diseases.
- It now equally emphasizes disease prevention and health promotion.
- The scope of medicine has expanded to address both individual health and community health problems.
Integration of Health Services
- Modern healthcare systems must integrate:
- Health promotion and disease prevention
- Curative care for acute conditions
- Long-term management of chronic diseases
- This integration should occur at all levels of the healthcare system.
- The goal is to ensure equitable, efficient, and high-quality healthcare delivery for the entire population.
Role of Health Systems
- Progress in health depends on strong and well-organized health systems.
- Primary Health Care (PHC) remains the cornerstone for achieving comprehensive health services.
- PHC supports accessibility, community participation, and continuity of care.
Future Perspective
- Medicine continues to evolve in response to scientific advances and societal needs.
- Ongoing development will be shaped by efforts to achieve better health outcomes and equity.
- Future generations will evaluate current achievements and limitations, guiding further progress.
- The evolution of medicine reflects humanity’s continuous pursuit of improved health and well-being.
Important Questions
- Explain how medicine evolved from primitive practices to modern scientific medicine.
- Describe the development of germ theory. Highlight contributions of Louis Pasteur and Robert Koch.
- What is meant by the tridosha theory in Ayurveda?
- Name the three doshas and their corresponding elements.
- What is the basic concept of yin and yang in Chinese medicine?
- Who is known as the Father of Medicine, and why?
- What is the significance of the Public Health Act of 1848?
