Competencies
- AN43.4: Describe the development and developmental basis of congenital anomalies of face, palate, tongue (included in this chapter), branchial apparatus, pituitary gland, thyroid gland, eye.
- AN39.1: Describe the embryological basis of nerve supply of tongue.
The mouth cavity and its associated structures begin forming very early in embryonic life through a complex but well-organized sequence of developmental events. Small epithelial thickenings, tissue swellings, and migrating cells gradually shape the oral cavity, teeth, tongue, and salivary glands. Understanding these developmental processes explains not only how the normal oral structures are formed but also why certain congenital anomalies of the mouth and teeth occur.
DEVELOPMENT OF MOUTH CAVITY
The mouth cavity develops through contributions from two embryonic germ layers: ectoderm and endoderm.
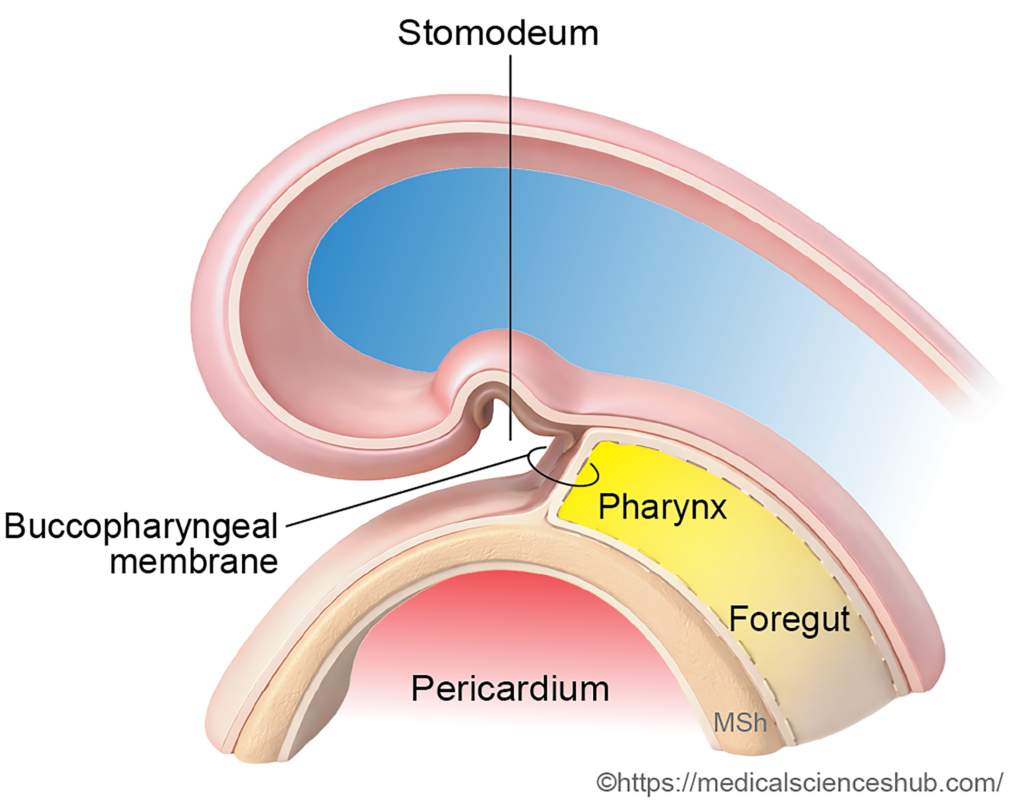
- The ectoderm forms the stomodeum, which represents the primitive oral cavity.
- The endoderm of the cephalic foregut contributes to the definitive oral cavity.
During the fourth week of development, the buccopharyngeal membrane ruptures. This event establishes continuity between the ectoderm of the stomodeum and the endoderm of the foregut, thereby forming a continuous oral passage.
Primitive Oral Cavity
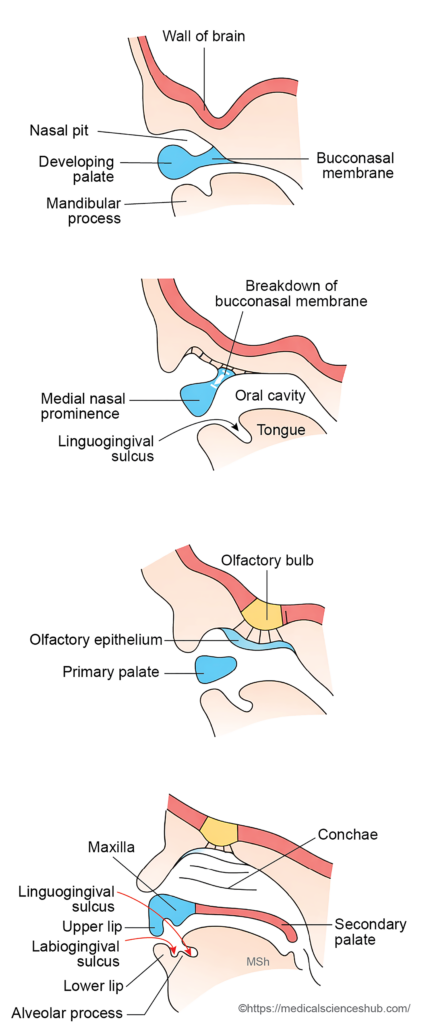
The primitive oral cavity originates from the stomodeum and is lined by ectoderm. As development proceeds, the growing palate divides the stomodeum into nasal and oral regions.
- The nasal part gives rise to the mucous membrane of the nasal cavity, the nasal septum, and the palate.
- The oral part forms the mucous membrane of the lips, cheeks, gums, and the enamel of the teeth.
Definitive Oral Cavity
- The definitive oral cavity develops mainly from the endodermal lining of the foregut.
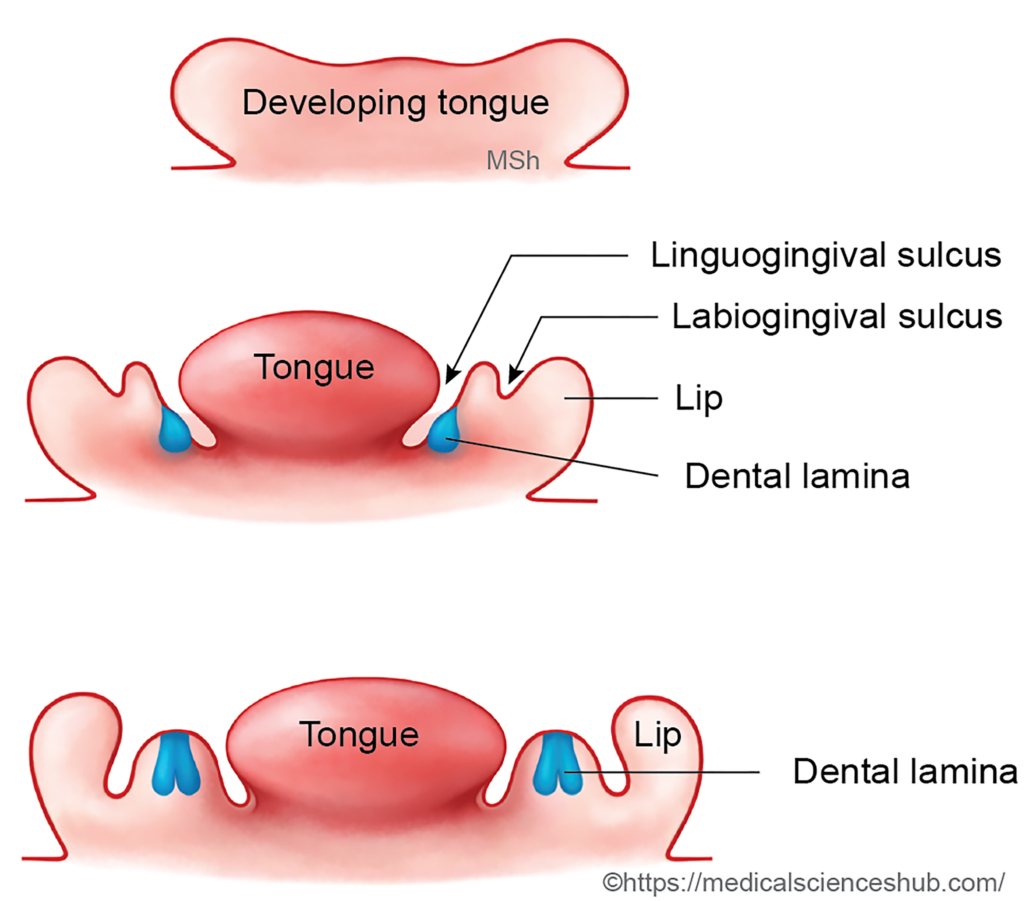
- Within the floor of the oral cavity, the developing tongue becomes separated from the mandibular process by the linguogingival sulcus, which marks the endodermal zone.
- Lateral to this groove, an ectodermal zone forms the labiogingival sulcus, which gradually deepens during development.
- Growth of the mandibular arch produces the lower lip, the lower portions of the cheeks, and the mandible.
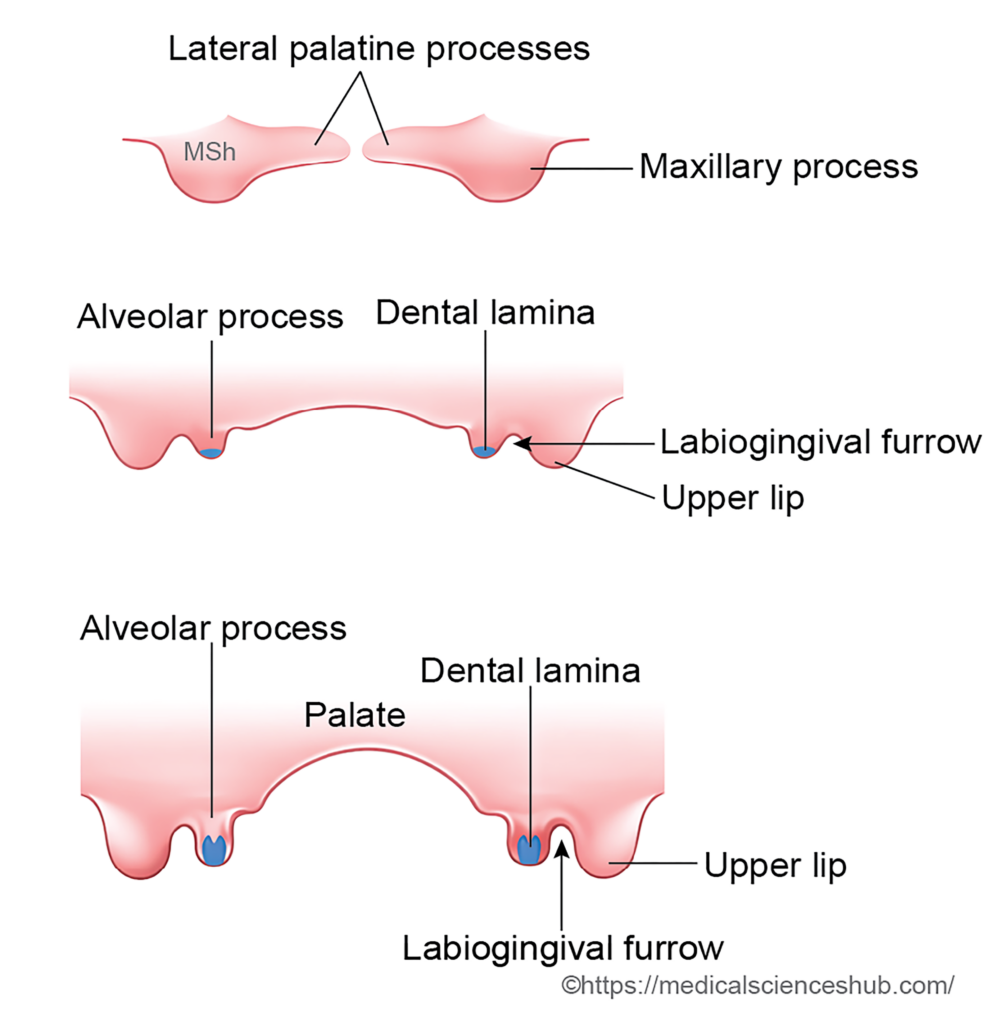
- The tissue located between the linguogingival sulcus and the labiogingival sulcus elevates to form the alveolar process, which later supports the teeth and jaw structures.
- In the upper region, the upper lip becomes separated from the developing alveolar process by the labiogingival furrow.
DEVELOPMENT OF TEETH
Humans develop two sets of teeth during life:
- Deciduous (milk) teeth – 20 in number.
- Permanent teeth – 32 in number.
Permanent incisors, canines, and premolars are termed successional teeth because they replace the corresponding milk teeth. In contrast, permanent molars are superadded teeth, as they develop without replacing any deciduous teeth.
Source of Development
Each tooth originates from two embryonic tissues:
- Surface ectoderm, which forms the enamel.
- Ectomesenchyme derived from neural crest cells, which forms dentine, pulp, cementum, and the periodontal ligament.
Structure of a Tooth
A mature tooth consists of the following main components:
- Enamel
- Dentine
- Cementum
- Pulpandperiodontal ligament
Stages of Tooth Development
Tooth formation proceeds through a series of well-defined stages.
1. Dental lamina stage
During the 6th week of development, the oral epithelium in the region of the developing alveolar process thickens to form a U-shaped epithelial band called the dental lamina
2. Bud stage
Localized proliferations appear at ten sites in each alveolar process. These epithelial thickenings grow into the underlying mesenchyme and form tooth buds, which represent the early enamel organs.
3. Cap stage
By the 8th week, the enamel organ enlarges and becomes cap-shaped. A condensation of mesenchymal cells, largely derived from neural crest, forms the dental papilla within the concavity of the enamel organ.
4. Bell stage
Further growth produces a bell-shaped enamel organ. Cells of the inner dental epithelium differentiate into ameloblasts, which produce enamel. Adjacent cells of the dental papilla differentiate into odontoblasts, which later form dentine. The enamel organ now shows three layers:
- Outer dental epithelium
- Inner dental epithelium (ameloblast layer)
- Stellate reticulum, a loose central cell network.
5. Apposition stage
Hard tissues begin to form. Ameloblasts deposit enamel on the outer surface of the basement membrane, while odontoblasts deposit dentine on its inner surface. As dentine forms, odontoblast processes (Tomes’ processes) extend into the dentinal tubules. Continued dentine deposition gradually narrows the pulp cavity, leaving a pulp canal through which nerves and blood vessels enter the tooth.
Mesenchymal cells surrounding the developing root differentiate into cementoblasts, which produce cementum. Surrounding connective tissue forms the periodontal ligament, anchoring the tooth root to the alveolar bone. A thin Nasmyth’s membrane (dental cuticle) may temporarily cover the enamel surface.
6. Eruption stage
Elongation of the tooth root and remodeling of surrounding tissues gradually move the tooth toward the oral cavity, resulting in tooth eruption. The timing of eruption varies among different teeth.
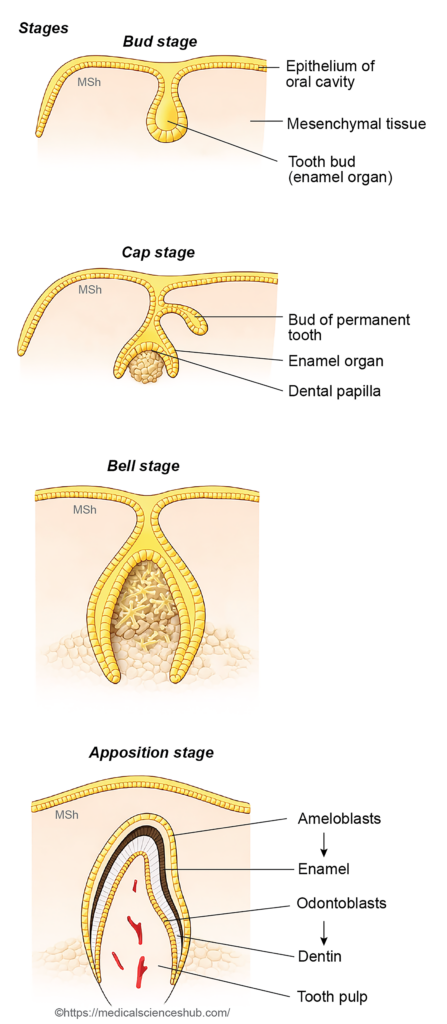
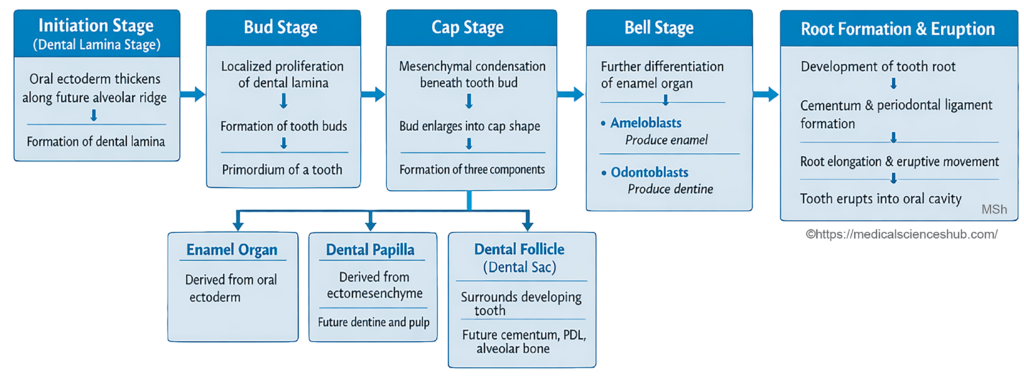
Table 12.1: Chronology of Tooth Eruption in Humans
| Dentition Type | Tooth | Typical Age of Eruption |
|---|---|---|
| Primary Dentition (Deciduous) | Mandibular Central Incisors | 6–9 months |
| Maxillary Central Incisors | 8–10 months | |
| Mandibular Lateral Incisors | 10–16 months | |
| First Primary Molars | 12–16 months | |
| Primary Canines (Cuspids) | 16–20 months | |
| Second Primary Molars | 20–30 months | |
| Permanent Dentition | First Permanent Molars | 6–7 years (often the first permanent teeth to erupt) |
| Central Incisors | 7–8 years | |
| Lateral Incisors | 8–9 years | |
| First Premolars | 10–11 years | |
| Canines | 10–12 years | |
| Second Premolars | 11–12 years | |
| Second Molars | 11–13 years | |
| Third Molars (Wisdom Teeth) | 18–25 years, though eruption may be delayed or absent |
Development of Permanent Teeth
- Humans normally develop 32 permanent teeth, which gradually replace the primary (deciduous) teeth and also include additional posterior teeth.
- Around the third month of intrauterine life, small epithelial outgrowths known as tooth buds arise from the dental lamina on the lingual side of the developing deciduous teeth. These buds remain inactive for several years after birth.
- Later, typically between 6 and 7 years of age, they begin to grow and differentiate to form the permanent incisors, canines, and premolars.
- As each permanent tooth develops and enlarges, it exerts pressure on the root of the corresponding deciduous tooth, leading to root resorption and eventual shedding of the primary tooth.
- The permanent molars differ in origin. Their tooth buds also develop from the dental lamina, but they arise posterior to the primary dentition rather than from the lingual side of existing teeth. These buds remain inactive until the time approaches for molar eruption.
- Enamel is the hardest tissue in the human body, while dentin is the second hardest calcified tissue and forms the bulk of the tooth structure.
CLINICAL EMBRYOLOGY
Anomalies of Teeth
Several developmental abnormalities can affect the number, structure, and eruption of teeth.
- Anodontia refers to the complete congenital absence of teeth, resulting from failure of tooth germ formation.
- Supernumerary teeth are extra teeth beyond the normal number. Their presence may disturb normal alignment and lead to malocclusion.
- Natal teeth are teeth present at birth. They usually represent prematurely erupted primary teeth.
- Gemination (often confused with fusion) occurs when a single tooth germ partially divides, producing a tooth with a widened crown that may appear as two teeth.
- Tooth impaction describes the failure of a tooth to erupt into the oral cavity due to obstruction or lack of space. The third molar (wisdom tooth) is the most frequently impacted tooth.
- Amelogenesis imperfecta is a hereditary disorder affecting enamel formation, resulting in thin, soft, or poorly mineralized enamel that may appear yellowish-brown and fragile.
- Dentinogenesis imperfecta is an autosomal dominant condition associated with mutations commonly involving chromosome 4 (4q). The dentin is abnormal, causing fragile teeth in which enamel fractures easily and dentin becomes exposed.
- A dentigerous cyst develops around the crown of an unerupted tooth, most often associated with an impacted permanent tooth.
DEVELOPMENT OF TONGUE
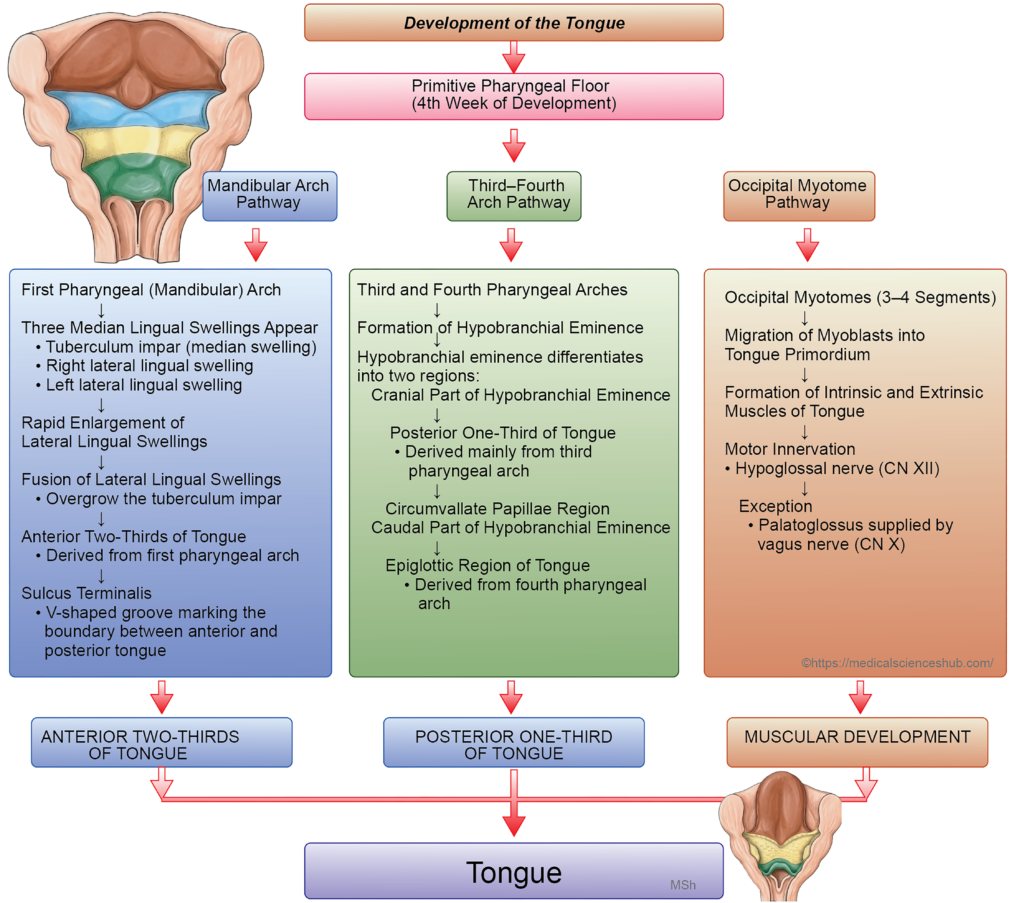
The tongue develops in the floor of the primitive pharynx and the developing oral cavity during early embryonic life. Its formation involves coordinated contributions from several embryonic tissues. The tongue is derived from three principal sources:
- Endoderm lining the pharyngeal arches forms the mucous membrane that covers most of the tongue surface.
- Mesenchyme associated with the pharyngeal arches develops into the fibro-areolar connective tissue (stroma) of the tongue.
- Occipital myotomes give rise to the intrinsic and extrinsic muscles of the tongue. These migrating muscle precursors carry their nerve supply from the hypoglossal nerve (cranial nerve XII).
Mucous Membrane of tongue
- The mucous membrane of the tongue develops from structures associated with the pharyngeal arches in the floor of the primitive pharynx.
- During the fourth week, the mandibular (first) arch shows three elevations: a single median swelling called the tuberculum impar and two lateral lingual swellings.
- The lateral swellings enlarge rapidly and fuse with each other and with the tuberculum impar. This fusion forms the anterior two-thirds of the tongue.
- As development proceeds, the alveololingual sulcus forms and gradually separates the tongue from the floor of the mouth.
- Posterior to the tuberculum impar, epithelial proliferation forms the thyroglossal duct. Its opening in the pharynx is represented by a small depression known as the foramen caecum, which marks the site of origin of the thyroid diverticulum.
- In the region of the third and fourth pharyngeal arches, a median swelling called the hypobranchial eminence (also known as the copula of His) appears during the fifth week.
- The ventral part of this structure enlarges to form the posterior one-third of the tongue, while the caudal part contributes to the epiglottis.
- The line of fusion between the anterior and posterior parts of the tongue is indicated by the sulcus terminalis.
- Some cells from the posterior region migrate forward across the sulcus terminalis to form the circumvallate papillae. During this period, the third arch overgrows the second arch and fuses with the first arch, resulting in incorporation of the second arch mesoderm within the developing tongue.
Muscles of Tongue
- The muscles of the tongue originate from three to four occipital myotomes. Cells from these myotomes migrate ventrally into the mesenchyme of the developing tongue and differentiate to form both the intrinsic and extrinsic muscles of the tongue.
- During this migration, the muscle precursors carry their nerve supply, the hypoglossal nerve (cranial nerve XII).
- As a result, this nerve supplies nearly all tongue muscles and follows a characteristic course in the neck, passing superficially across the external and internal carotid arteries.
Nerve Supply of tongue
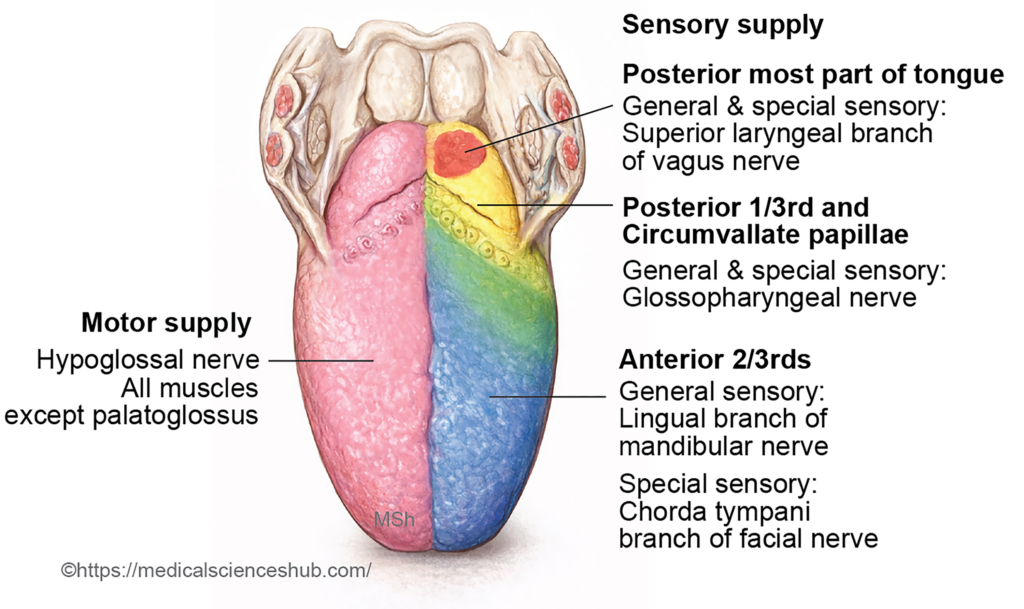
The nerve supply of the tongue reflects its embryological origin from different pharyngeal arches.
- The anterior two-thirds of the tongue develops from the first pharyngeal (mandibular) arch. Therefore, its general sensory innervation is provided by the lingual nerve, a branch of the mandibular division of the trigeminal nerve (CN V3). Taste sensation from this region is transmitted through the chorda tympani, a branch of the facial nerve (CN VII) that joins the lingual nerve.
- The posterior one-third of the tongue, including the circumvallate papillae, arises mainly from the third pharyngeal arch through the hypobranchial eminence. Consequently, both general sensation and taste from this region are supplied by the glossopharyngeal nerve (CN IX).
- The most posterior part of the tongue near the vallecula develops from the fourth pharyngeal arch. Sensory innervation in this region is provided by the internal laryngeal branch of the vagus nerve (CN X).
- The muscles of the tongue, except the palatoglossus, originate from occipital myotomes and are therefore innervated by the hypoglossal nerve (CN XII). The palatoglossus muscle receives motor supply from the vagus nerve through the pharyngeal plexus.
CLINICAL EMBRYOLOGY
Developmental Anomalies of Tongue
Several congenital abnormalities of the tongue arise from disturbances during embryonic development.
- Aglossia – a rare condition characterized by complete absence of the tongue due to failure of its formation.
- Hemiglossia – partial absence of the tongue resulting from defective development of one lateral lingual swelling, producing an incomplete half of the tongue.
- Bifid tongue – a cleft or split anterior tongue caused by failure of fusion of the two lateral lingual swellings during development.
- Ankyloglossia (tongue-tie) – occurs when the lingual frenulum remains abnormally short because of incomplete formation of the alveololingual sulcus, restricting tongue movement.
- Microglossia and macroglossia – abnormal tongue size, where the tongue is unusually small or excessively enlarged, respectively.
- Ankyloglossia superior – a rare condition in which the tongue is abnormally attached to the palate, limiting its mobility.
- Lingual thyroid – results from failure of the thyroid gland to descend from the foramen caecum, leaving thyroid tissue at the base of the tongue.
Table 12.2: Embryological Origin and Nerve Supply of the Tongue
| Region/Structure of the Tongue | Embryological Origin | Primary Nerve Supply |
|---|---|---|
| Mucosa of the Anterior Two-Thirds | Develops mainly from the first pharyngeal arch, formed by the lateral lingual swellings and the tuberculum impar. | General sensation: Lingual nerve (branch of the mandibular division of the trigeminal nerve – V3). Taste sensation: Chorda tympani branch of the facial nerve (VII). |
| Mucosa of the Posterior One-Third (includingcircumvallate papillae) | Derived from the third pharyngeal arch. | General and taste sensation: Glossopharyngeal nerve (IX). |
| Posterior-most part of the Tongue (near the epiglottis) | Arises from the fourth pharyngeal arch. | General and taste sensation: Internal laryngeal branch of the superior laryngeal nerve, a branch of the vagus nerve (X). |
| Intrinsic and Extrinsic Tongue Muscles | Develop from migrating muscle cells of the occipital myotomes. | Motor supply: Hypoglossal nerve (XII) to all tongue muscles except the palatoglossus, which is supplied by the vagus nerve (X) via the pharyngeal plexus. |
Development of Salivary Glands
- Humans possess three paired major salivary glands: the parotid, submandibular, and sublingual glands. Their epithelial components arise from the oral cavity lining.
- The parotid gland develops from ectoderm, whereas the submandibular and sublingual glands originate mainly from endoderm.
- All salivary glands begin as epithelial outgrowths from the oral mucosa.
- These outgrowths form solid epithelial cords that grow into the surrounding mesenchyme.
- With further development, the cords undergo canalization to form ducts and repeatedly branch to produce smaller ducts.
- The terminal ends differentiate into secretory units called acini.
- The primary canalized cord forms the main excretory duct, and its opening into the oral cavity appears as a ductal papilla.
- Humans possess three paired major salivary glands: the parotid, submandibular, and sublingual glands. Their epithelial components arise from the oral cavity lining.
- The parotid gland develops from ectoderm, whereas the submandibular and sublingual glands originate mainly from endoderm.
- All salivary glands begin as epithelial outgrowths from the oral mucosa.
- These outgrowths form solid epithelial cords that grow into the surrounding mesenchyme.
- With further development, the cords undergo canalization to form ducts and repeatedly branch to produce smaller ducts.
- The terminal ends differentiate into secretory units called acini.
- The primary canalized cord forms the main excretory duct, and its opening into the oral cavity appears as a ductal papilla.
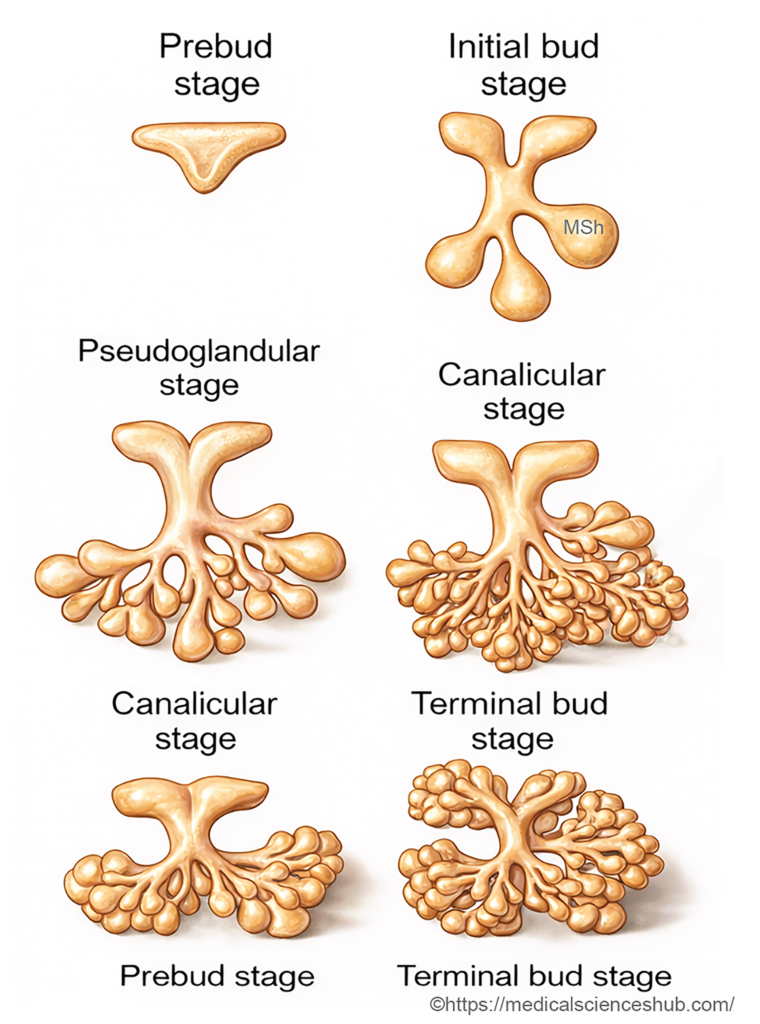
- Developmental Stages: The formation of salivary glands proceeds through several recognizable stages: prebud stage, initial bud stage, pseudoglandular stage, canalicular stage, and finally the terminal bud stage, during which functional secretory units are established.
Parotid Gland
- The parotid gland begins to develop during the fifth week as an ectodermal epithelial outgrowth from the cheek near the angle of the stomodeum, between the maxillary and mandibular processes.
- This epithelial groove later canalizes to form the parotid duct.
- The distal end of the duct proliferates and branches to produce ductules and acini.
- Fusion of the maxillary and mandibular processes reduces the oral fissure and increases the length of the duct.
- In the adult, the parotid duct opens into the oral vestibule opposite the upper second molar tooth.
- The presence of myoepithelial cells around parotid acini supports its ectodermal origin.
Submandibular Gland
- The submandibular gland develops during the sixth week from an endodermal epithelial outgrowth arising in the floor of the mouth near the alveololingual groove.
- This epithelial cord later canalizes to form the submandibular duct, while its terminal branches differentiate into secretory acini and ductules.
Sublingual Gland
- The sublingual gland develops slightly later, around the seventh week, from several endodermal epithelial buds arising from the linguogingival sulcus and the region near the submandibular duct.
- These multiple buds form numerous small ducts that eventually constitute the sublingual gland.
DEVELOPMENT OF PHARYNX
- The pharynx develops from the cranial part of the foregut during early embryonic life and forms a common passage for both the respiratory and digestive systems.
- The lateral walls and floor of the developing pharynx give rise to a series of pharyngeal pouches, which later differentiate into several important structures of the head and neck.
- In the floor of the pharynx, just caudal to the hypobranchial eminence, a median depression called the laryngotracheal groove (furcula of His) appears. This groove deepens to form a respiratory diverticulum, which later develops into the larynx, trachea, bronchi, and lungs.
- Subsequent formation of the nose, palate, and the respiratory diverticulum divides the pharynx into three anatomical regions: the nasopharynx, oropharynx, and laryngopharynx.
- Occasionally, a small cystic remnant known as the pharyngeal bursa (pouch of Luschka) may be present in the posterior wall of the nasopharynx, near the lower part of the pharyngeal tonsil. This structure represents a notochordal remnant.
Important Questions
- Describe the stages involved in the development of teeth.
- Enumerate the sequence of eruption of deciduous (temporary) and permanent teeth.
- Write a short note on the embryological development of the tongue.
- Explain the correlation between the embryological origin of the tongue and its nerve supply..
