Competencies
- AN52.8: Describe the development of male and female reproductive system.
INTRODUCTION
- The genital system comprises the gonads and genital ducts. The gonads include the testes in males and ovaries in females. They originate from the genital ridge, which forms through the proliferation of coelomic epithelium and incorporation of primordial germ cells (PGCs).
- The male genital ducts develop into the efferent ductules, epididymis, vas deferens, seminal vesicles, and ejaculatory ducts. In females, the genital ducts give rise to the uterine tubes, uterus, and vagina.
The accessory sex glands include the prostate and bulbourethral glands in males, and the greater vestibular (Bartholin’s) glands in females. - During early embryonic life, two paired duct systems are present: the mesonephric (Wolffian) ducts and paramesonephric (Müllerian) ducts. Depending on sex differentiation, one system develops while the other regresses, ultimately forming the definitive genital duct system.
Primordial germ cells
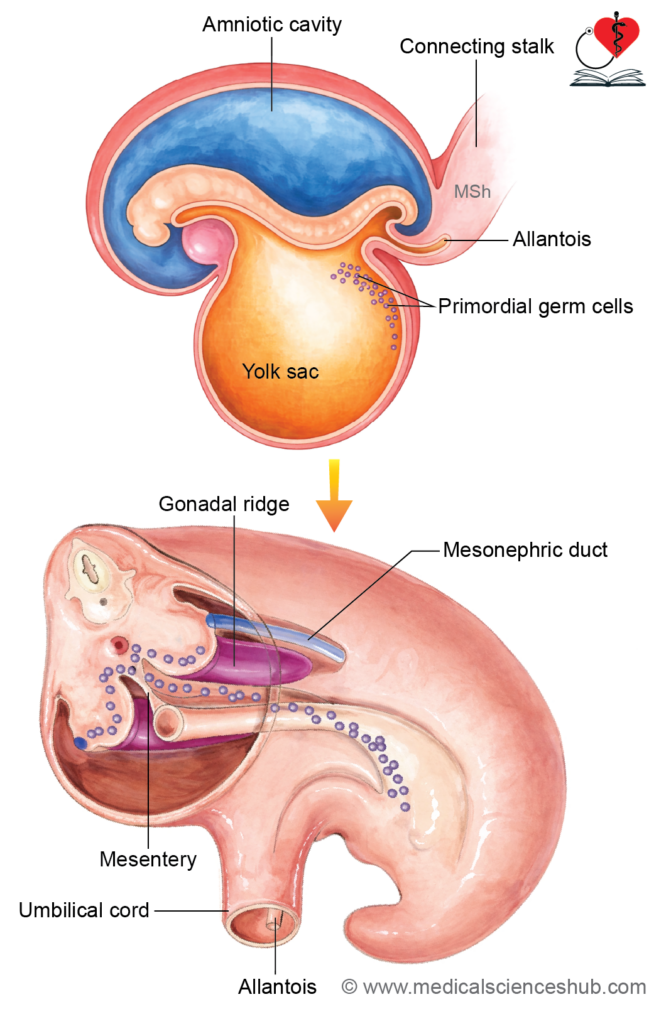
- Primordial germ cells (PGCs) originate from the epiblast during the second week of development. They temporarily reside in the extraembryonic mesoderm of the yolk sac wall and connecting stalk. With embryonic folding, they become positioned within the splanchnopleuric mesoderm surrounding the hindgut.
- By the fifth week, the coelomic epithelium overlying the mesonephric ridge proliferates to form the genital ridges, marking the initial stage of gonadal development. At this time, PGCs migrate bilaterally from the yolk sac to the genital ridges via the dorsal mesentery, using amoeboid movement, where they contribute to gonad formation.
FORMATION OF PRIMITIVE GONADS
Genital Ridge (Gonadal Ridge)
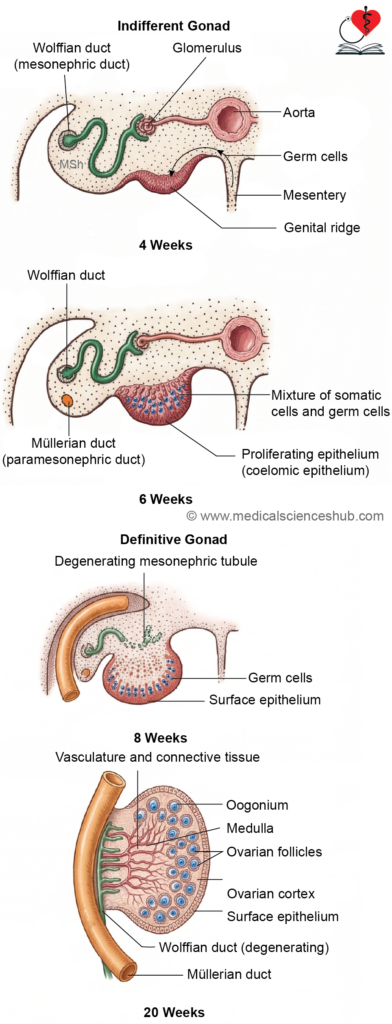
- In the fifth week of development, the coelomic epithelium lining the primitive peritoneal cavity proliferates over the medial surface of the mesonephros, forming the genital ridge. The genitourinary system originates from this region of intermediate mesoderm.
- The genital ridge appears as a longitudinal elevation on the posterior abdominal wall, located between the dorsal aorta and the mesonephros. It differentiates into an outer cortex and inner medulla.
- Both testes and ovaries develop from the genital ridge and initially lie retroperitoneally in the lumbar region, approximately at the T10 level.
Migration of Primordial Germ Cells
- During the fourth week, primordial germ cells (PGCs) migrate from the yolk sac to the genital ridge via the dorsal mesentery. Their arrival is essential for normal gonadal development.
Formation of primitive sex cords
- The coelomic epithelium gives rise to multiple epithelial projections that grow into the underlying mesenchyme of the genital ridge. These projections form solid, finger-like structures known as primitive sex cords, which represent the earliest stage in the differentiation of gonadal tissue.
Differentiation into Definitive Gonad
- Up to the 7th week of intrauterine life, the gonad remains indifferent (ambisexual). Its differentiation into a testis or ovary depends on the chromosomal sex of the embryo.
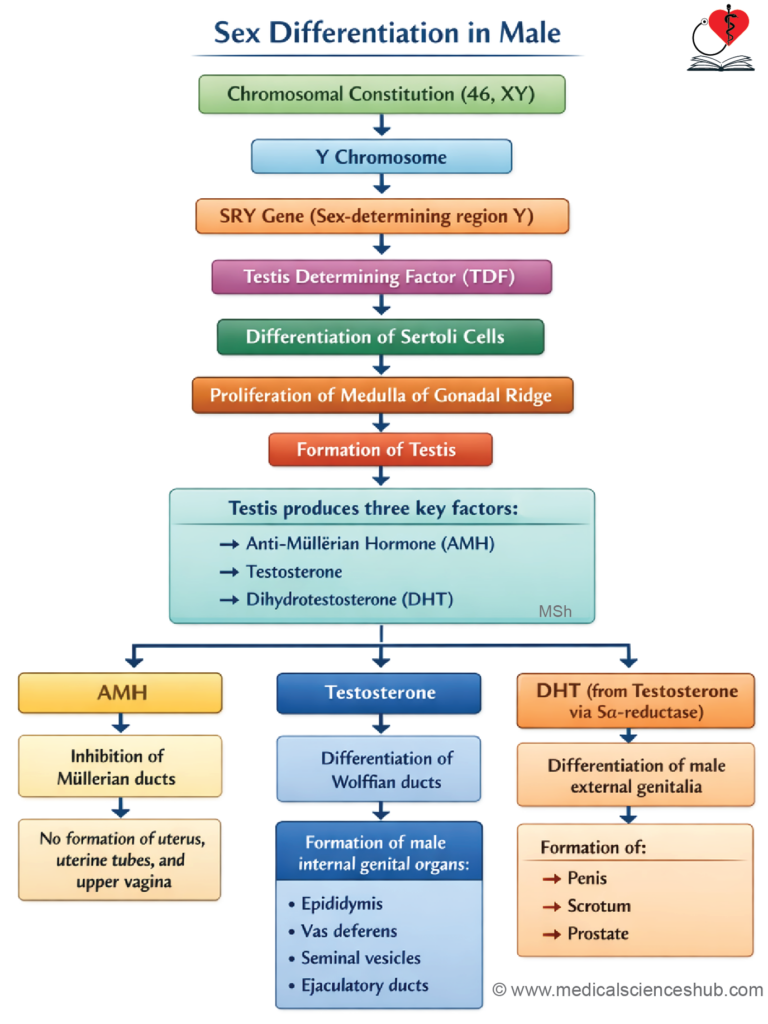
- In individuals with a Y chromosome, the SRY gene (sex-determining region of Y) produces the testis-determining factor (TDF). This factor initiates the differentiation of Sertoli cells, which secrete anti-Müllerian hormone (AMH).
- AMH causes regression of the paramesonephric (Müllerian) ducts, thereby preventing female duct development.
- TDF also promotes the formation of Leydig cells, which begin secreting testosterone and dihydrotestosterone (DHT) from around the 8th week.
- Testosterone supports development of the mesonephric ducts into male genital structures, while DHT is essential for the formation of external male genitalia and the prostate.
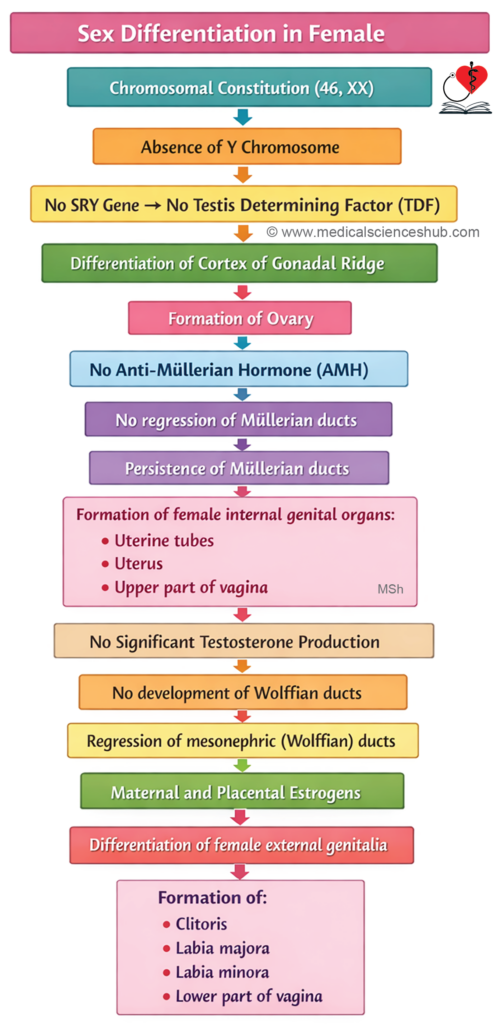
- In the absence of the SRY gene and TDF, the gonad develops into an ovary. The primitive sex cords give rise to follicular cells, and the cortex develops while the medulla regresses. Formation of normal ovarian follicles requires activity of both X chromosomes initially; later, one X chromosome becomes inactivated as a Barr body.
- Structurally, the genital ridge consists of an outer cortex and inner medulla. In males, the medulla differentiates into the testis and the cortex regresses, whereas in females, the cortex forms the ovary and the medulla degenerates.
- In the absence of androgens, the Müllerian ducts develop into the uterine tubes and uterus, influenced by maternal and placental estrogens, which also promote formation of female external genitalia.
DEVELOPMENT OF TESTIS
The testis is the male gonad, and its components arise from different embryological structures:
- Medulla of the genital ridge gives rise to the seminiferous tubules, rete testis, interstitial (Leydig) cells, fibrous septa, and intrinsic coverings of the testis.
- Mesonephric tubules (approximately 12–15) differentiate into the efferent ductules, which connect the testis to the epididymis.
- The mesonephric (Wolffian) duct forms the epididymal canal and the vas deferens.
- The paramesonephric (Müllerian) duct largely regresses, leaving small vestigial remnants such as the appendix of the testis.
- The mesonephros itself undergoes degeneration, with residual structures persisting as the appendix of the epididymis.
This coordinated development ensures proper formation of the male reproductive system and its ductal connections.
Stages of Development of Testis
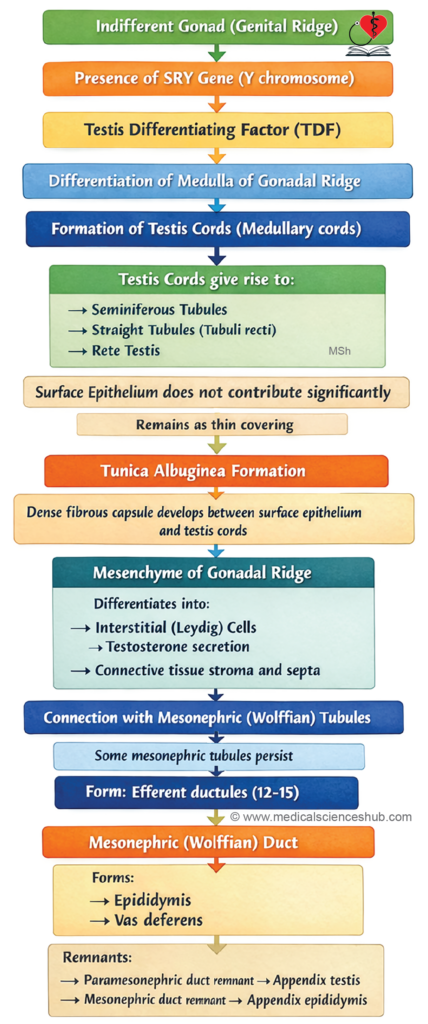
- The development of the testis is initiated by the testis-determining factor (TDF), produced by the SRY gene on the short arm of the Y chromosome.
- The testis arises from the medulla of the genital ridge. Here, primitive sex cords proliferate and extend inward to form medullary cords, which grow toward the hilum of the developing testis. Near the hilum, these cords interconnect to form a network that later differentiates into the rete testis, while the cords themselves undergo canalization to become seminiferous tubules. Functional connections between these structures are established by the fourth month of intrauterine life.
- Cells derived from the coelomic epithelium differentiate into Sertoli cells, whereas primordial germ cells give rise to spermatogonia. By the seventh week, surrounding mesenchyme forms the tunica albuginea, along with mediastinal septa and Leydig cells.
- The rete testis establishes continuity with 12–15 mesonephric tubules, which become the efferent ductules. The mesonephric duct subsequently differentiates into the epididymis, vas deferens, seminal vesicles, and ejaculatory duct.
Descent of Testis
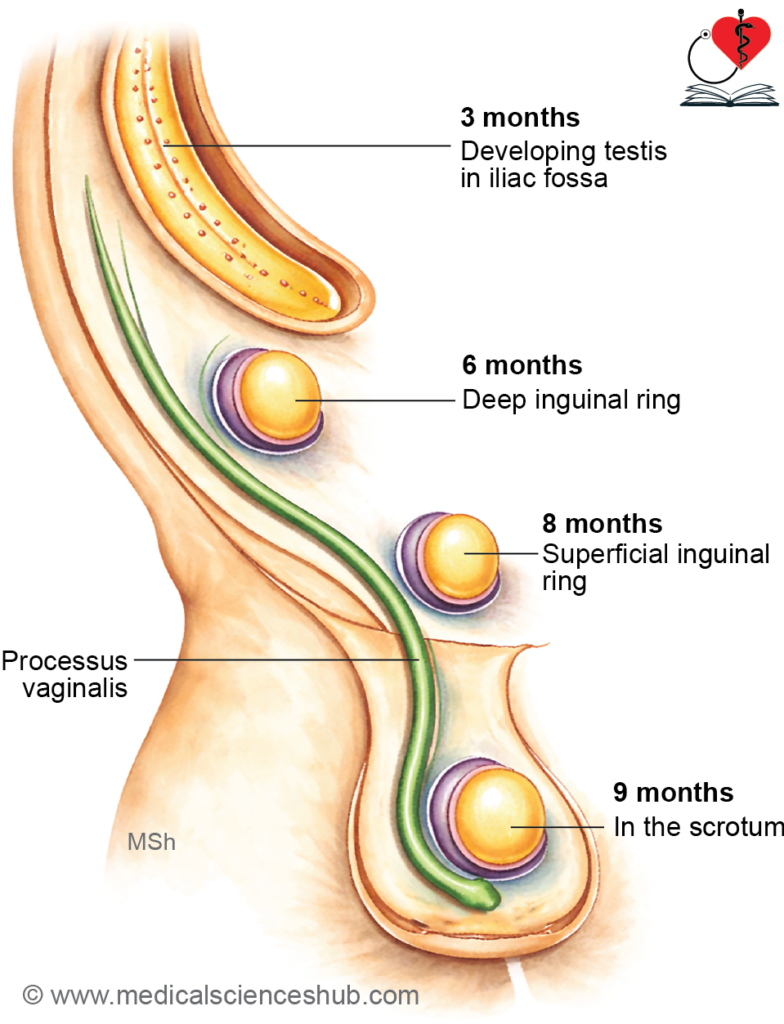
- The testis initially develops on the posterior abdominal wall at the level of the upper lumbar vertebrae. During fetal life, it gradually migrates downward to reach the scrotum, where it resides after birth outside the abdominal cavity.
- The descent occurs in a well-defined sequence:
- Third month: The testis reaches the iliac fossa.
- End of sixth month: It arrives at the deep inguinal ring.
- Seventh month: It passes through the inguinal canal.
- End of eighth month: It reaches the superficial inguinal ring.
- By the ninth month: It enters the scrotum.
- This process ensures proper positioning of the testes, which is essential for normal postnatal function, particularly spermatogenesis, as it requires a temperature lower than core body temperature.
Factors Responsible for Descent of Testis
The descent of the testis is a coordinated process influenced by multiple anatomical and hormonal factors:
- Differential growth
Rapid growth of the posterior abdominal wall relative to the testis contributes to its apparent downward movement. - Formation of the inguinal bursa
An outpouching of the anterior abdominal wall, called the inguinal bursa, extends outward. Its passage forms the inguinal canal, while the external swelling develops into the scrotum. - Gubernaculum testis
The gubernaculum is a mesenchymal cord connecting the inferior pole of the testis to the future scrotal region. As the body grows faster than the gubernaculum, the testis is guided downward. It also helps widen the inguinal pathway and directs the testis into the scrotum. - Processus vaginalis
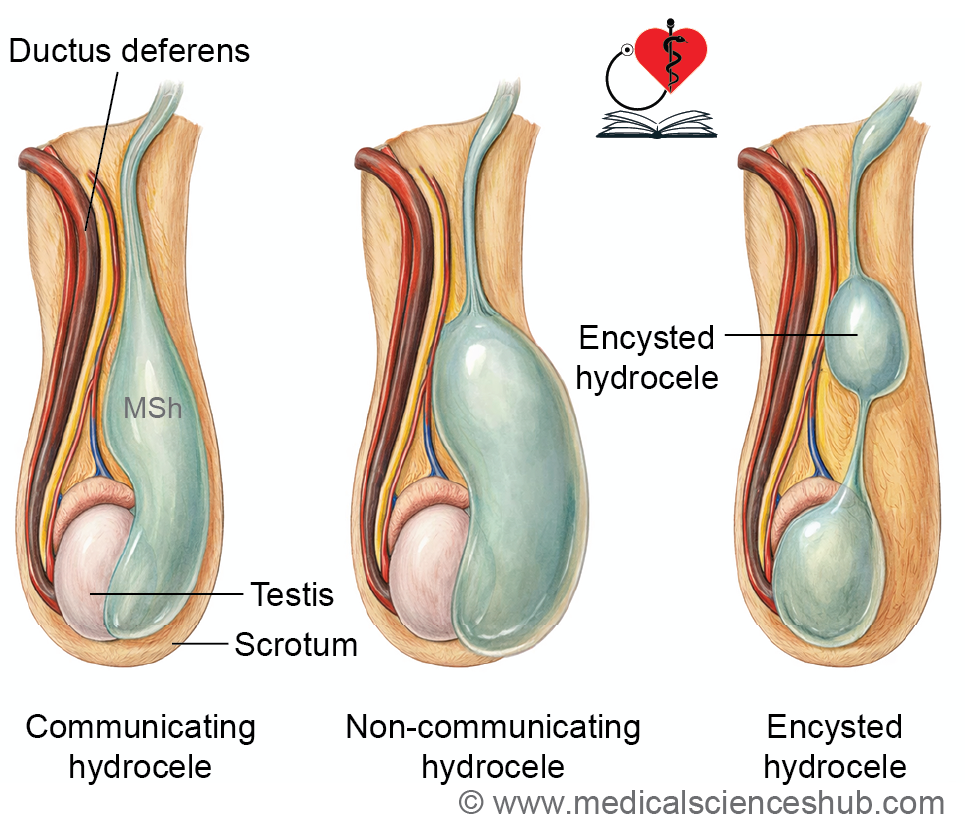
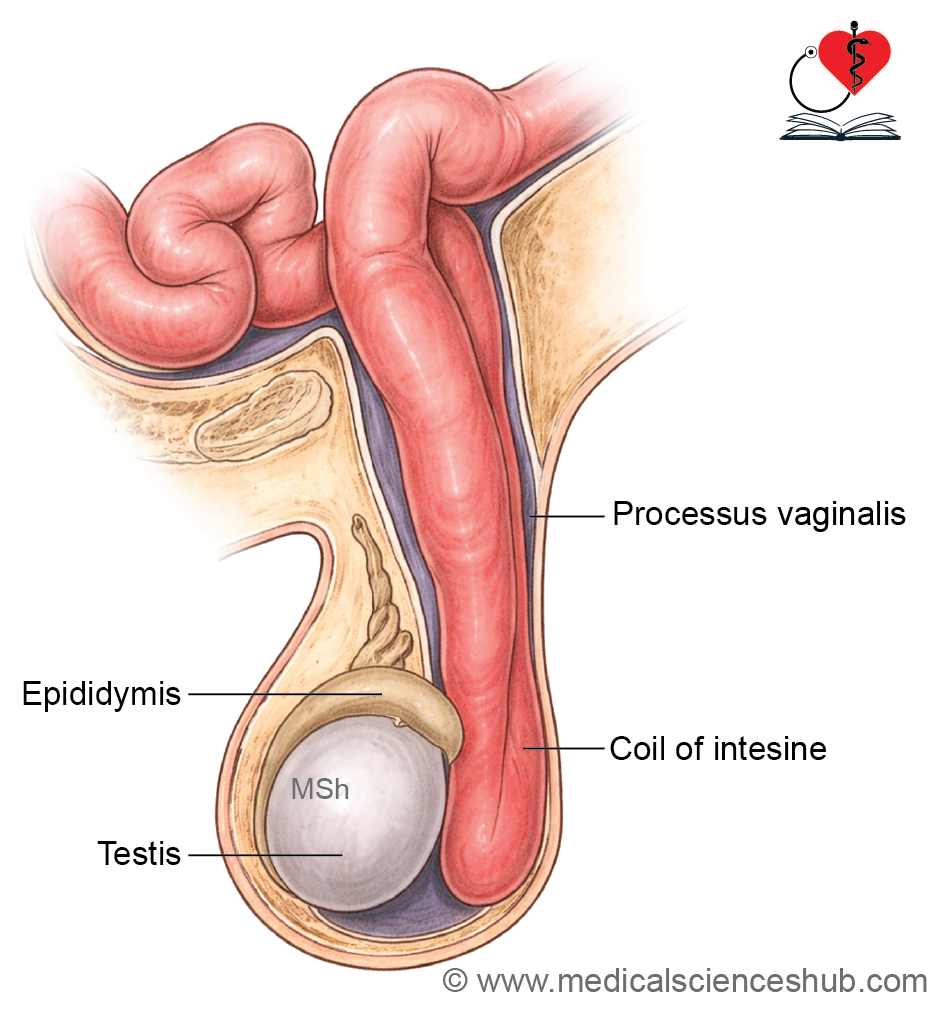
The processus vaginalis is a peritoneal diverticulum that precedes the testis through the inguinal canal into the scrotum. It facilitates testicular descent and later forms the tunica vaginalis. Its proximal portion normally obliterates under the influence of androgens, mediated partly by calcitonin gene-related peptide (CGRP) from the genitofemoral nerve and hepatocyte growth factor, while the distal part persists. - Additional factors
- Increased intra-abdominal pressure from enlarging viscera
- Influence of male sex hormones (androgens)
- Temperature difference between abdomen and scrotum
- Action of CGRP causing contraction of the cremaster muscle, aiding descent
These mechanisms act together to ensure proper positioning of the testes within the scrotum before birth.
CLINICAL EMBRYOLOGY
Anomalies of Testis
Common developmental abnormalities of the testis include:
- Cryptorchidism – failure of normal descent of one or both testes.
- Anorchism – complete absence or severe underdevelopment of both testes within the abdomen.
- Monorchism – only one testis descends, while the other remains intra-abdominal.
- Ectopic testis – deviation from the normal path of descent. It may be located in the perineum, anterior to the pubic symphysis, within the femoral canal, in the penile skin, or subcutaneously in the upper thigh.
- Congenital hydrocele and inguinal hernia – persistence of the processus vaginalis allows abdominal contents to herniate (inguinal hernia) or fluid to accumulate (hydrocele).
- Seminoma – a malignant germ cell tumor arising from primordial germ cells.
Cryptorchidism (undescended testis)
Definition
Cryptorchidism refers to incomplete descent of one or both testes, resulting in their absence from the scrotum.
Incidence
It occurs in approximately 3% of full-term and up to 30% of premature male infants. In nearly 80% of cases, spontaneous descent occurs within the first year of life.
Possible Locations
An undescended testis may be found at:
- Upper scrotum
- Superficial inguinal ring
- Inguinal canal
- Deep inguinal ring
- Iliac fossa or lumbar region
Clinical Features
- Infertility due to impaired spermatogenesis from higher intra-abdominal temperature
- Increased risk of malignancy and testicular atrophy
Management
- Observation during the first year, as spontaneous descent is common
- Orchidopexy, a surgical procedure to relocate the testis into the scrotum, if descent does not occur spontaneously
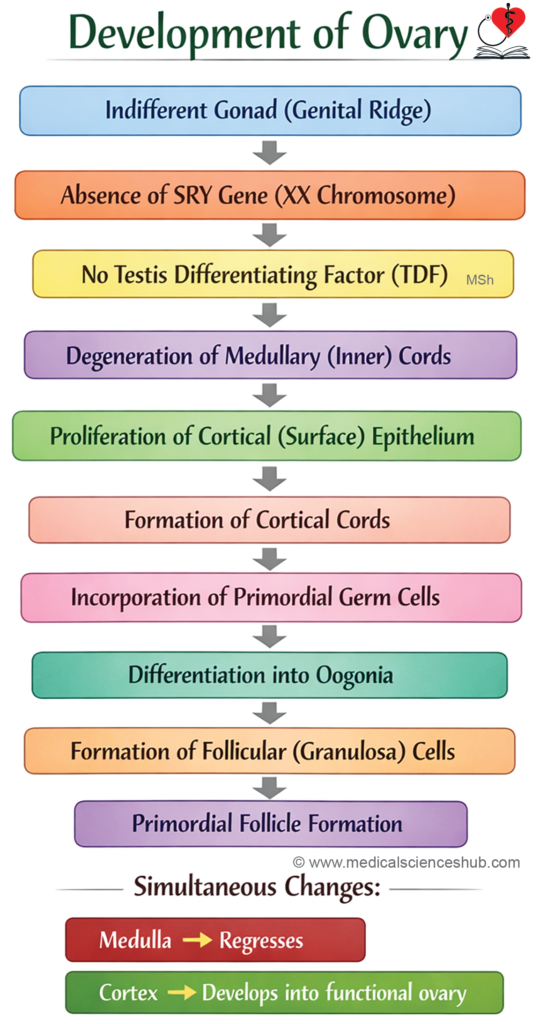
DEVELOPMENT OF OVARY
The ovaries are the female gonads, and their components arise from multiple embryological sources:
- Oocytes originate from primordial germ cells, which migrate from the yolk sac to the developing gonad.
- Follicular cells are derived from the cortical sex cords, which develop from the coelomic epithelium.
- The surface or germinal epithelium (simple cuboidal covering of the ovary) also arises from the coelomic epithelium of the genital ridge.
- The ovarian medulla forms from the regression of the medullary sex cords, leaving behind stromal tissue.
This coordinated differentiation results in the formation of a functional ovary with germ cells ad supporting structures.
Stages of Development of Ovary
- Primordial germ cells (PGCs) migrate from the yolk sac to the genital ridge, where they populate the developing ovary.
- The initial medullary sex cords degenerate, contributing to the formation of the ovarian medulla. By the seventh week, the coelomic epithelium forms a second generation of cords known as cortical cords, which remain confined to the cortex.
- By the third month, these cortical cords fragment into clusters that surround individual germ cells. The primordial germ cells differentiate into oogonia, while the surrounding cells become follicular cells, together forming primordial follicles.
- The ovarian surface is covered by a single layer of germinal epithelium, derived from coelomic epithelium. Despite its name, this layer does not produce germ cells.
- The ovary is attached to the posterior abdominal wall by a peritoneal fold called the mesovarium, which provides structural support.
This sequence ensures proper organization of germ cells and supporting elements within the developing ovary.
Descent of Ovary
The ovaries initially develop on the posterior abdominal wall and subsequently descend into the true pelvis, where they attain their final position.
Factors affecting descent of ovary
- Gubernaculum ovarii
The gubernaculum is a fibromuscular band extending from the inferior pole of the ovary to the genital swelling (future labium majus). It plays a key role in guiding ovarian descent. - Developing uterus and broad ligament
The descent of the ovary is limited by the formation of the uterus and broad ligament, as the gubernaculum becomes attached to the uterine angle. This results in stabilization of the ovary within the pelvis.
The gubernaculum subsequently differentiates into two structures:
- Ligament of ovary, connecting the ovary to the uterus
- Round ligament of uterus, which extends from the uterus to the labium majus through the inguinal canal
These factors ensure proper positioning of the ovaries within the pelvic cavity.
CLINICAL EMBRYOLOGY
Anomalies of Ovary
Developmental abnormalities of the ovary include:
- Structural variations
- Absence of one or both ovaries
- Duplication of the ovary
- Ectopic location, such as within the inguinal canal or labium majus
- Ovarian teratoma
This is a type of germ cell tumor composed of tissues derived from multiple germ layers. It may contain structures such as bone, cartilage, hair, or even tissues resembling thyroid or adrenal glands.
These anomalies arise from disturbances in normal gonadal development and germ cell differentiation.
PARAMESONEPHRIC (Müllerian) DUCTS
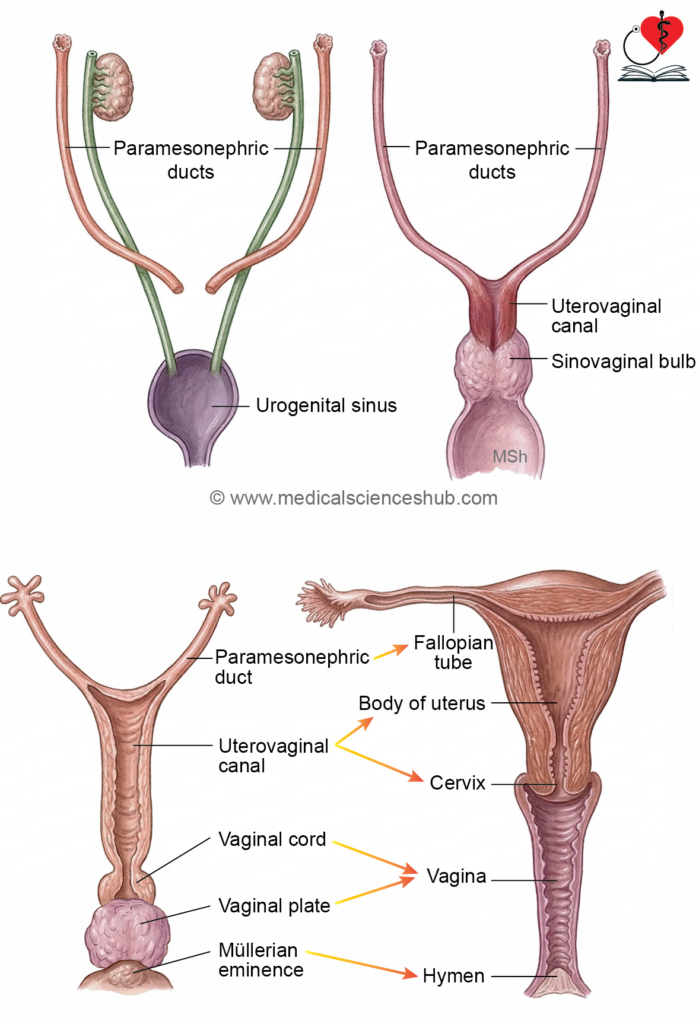
- The paramesonephric ducts develop during the 6th week from invaginations of the coelomic epithelium along the mesonephric ridge. Their cranial ends remain open to the coelomic cavity.
- By the 8th week, the caudal portions elongate, cross the mesonephric ducts anteriorly, and grow toward the urorectal septum. By the third month, the caudal segments of both ducts fuse to form the uterovaginal canal, which creates a projection in the dorsal wall of the urogenital sinus called the Müllerian tubercle.
Paramesonephric Ducts in Female
- The unfused cranial parts of each duct form the uterine tubes (fallopian tubes). Their openings into the coelomic cavity become the abdominal ostia, and surrounding mesenchyme contributes to fimbriae.
- The fused caudal parts form the uterovaginal canal. Its upper portion develops into the uterus, while the lower part contributes to the upper vagina.
- The caudal end of the uterovaginal canal projects into the urogenital sinus as the Müllerian tubercle. Adjacent proliferation forms a solid vaginal cord.
- From the urogenital sinus, paired sinovaginal bulbs develop and fuse to form the vaginal plate. This structure later canalizes (by the 5th month) to form the vaginal canal.
- Expansion around the cervix creates the vaginal fornices, while partial degeneration of the Müllerian tissue forms the hymen.
- The paramesonephric ducts give rise to the uterine tubes, uterus, upper part of the vagina, and vaginal fornices.
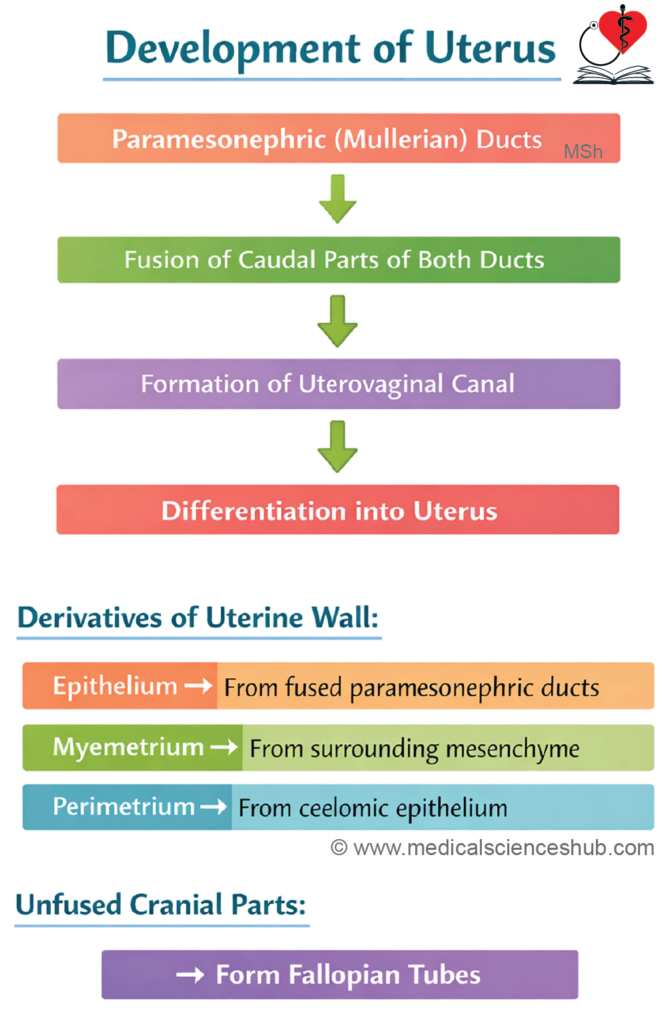
DEVELOPMENT OF UTERUS
- The uterus develops primarily from the uterovaginal canal, which is formed by fusion of the paramesonephric (Müllerian) ducts.
- The endometrial epithelium is derived from the lining of the uterovaginal canal.
- The myometrium and surrounding connective tissue arise from the adjacent mesoderm.
- The unfused cranial portions of the paramesonephric ducts differentiate into the uterine (fallopian) tubes.
- At birth, the cervix is relatively longer than the body of the uterus. After puberty, hormonal influences cause the body of the uterus to enlarge and exceed the cervix in length.
- This coordinated development ensures proper structural and functional maturation of the uterus.
CLINICAL EMBRYOLOGY
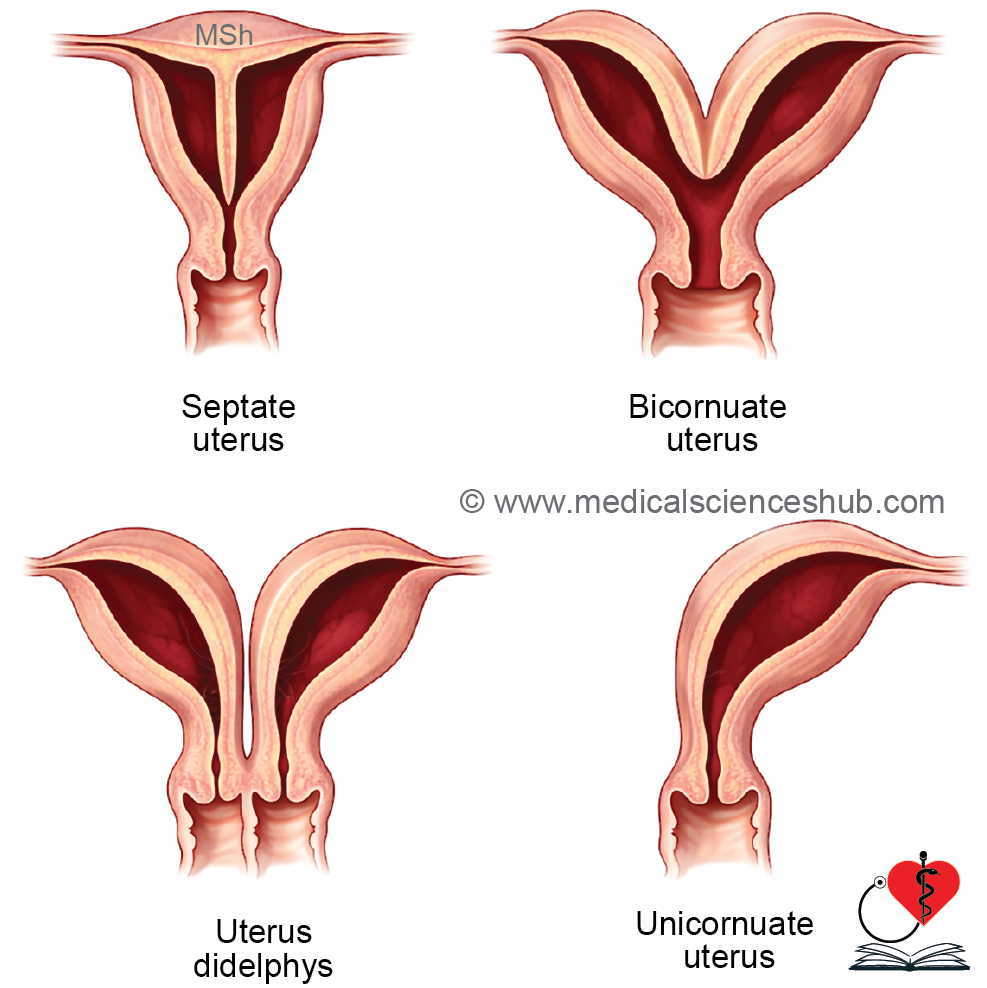
Anomalies of Uterus
Developmental abnormalities of the uterus arise mainly from defects in the fusion or canalization of the paramesonephric (Müllerian) ducts:
- Bicornuate uterus: Partial failure of fusion of the caudal Müllerian ducts results in a uterus with two horns (cornua), each connected to a fallopian tube.
- Unicornuate uterus: Failure of development of one Müllerian duct leads to a single-sided uterus with absence of the opposite uterine horn and tube.
- Septate uterus: Although fusion occurs, the intervening septum fails to resorb, dividing the uterine cavity.
- Uterine agenesis: Complete absence of the uterus due to failure of Müllerian duct development; this is a rare anomaly.
- Uterus didelphys (double uterus): Complete non-fusion of the Müllerian ducts produces two separate uterine cavities, each with its own cervix.
- Double uterus with double vagina: Combined failure of fusion of both the paramesonephric ducts and sinovaginal bulbs results in duplication of the uterus and vagina.
These anomalies can affect reproductive function and may present clinically with infertility or menstrual abnormalities.
DEVELOPMENT OF VAGINA
The vagina develops from both endodermal and mesodermal sources, with contributions differing above and below the hymen:
- Upper three-fourths (above hymen):
The epithelial lining (mucosa) originates from the sinovaginal bulbs of the urogenital sinus (endoderm). Surrounding muscle and connective tissue develop from mesoderm associated with the paramesonephric (Müllerian) ducts. - Lower one-fourth (below hymen):
This portion arises directly from the urogenital sinus (endoderm). - External vaginal orifice:
Formed from the genital folds following rupture of the urogenital membrane. - Hymen:
Derived from the Müllerian eminence, representing a thin membrane at the junction of the vaginal components.
This dual origin explains the structural and developmental differences between the upper and lower parts of the vagina.
CLINICAL EMBRYOLOGY
Congenital Anomalies of Vagina
- Imperforate hymen:
Results from failure of canalization of the central part of the Müllerian eminence, leading to persistence of the hymenal membrane. - Vaginal atresia:
Occurs due to incomplete or absent canalization of the vaginal plate, causing obstruction of the vaginal lumen. - Vaginal agenesis:
Characterized by absence of the vagina, due to failure of formation of the vaginal plate from the sinovaginal bulbs. - Septate vagina:
Develops from incomplete or irregular breakdown of the central tissue of the sinovaginal bulbs, resulting in a longitudinal or transverse septum. - Rectovaginal or vesicovaginal fistula:
Arises when the Müllerian eminence abnormally extends into the primitive rectum or vesicourethral canal, creating an abnormal communication.
These anomalies reflect defects in canalization, fusion, or partitioning during vaginal development.
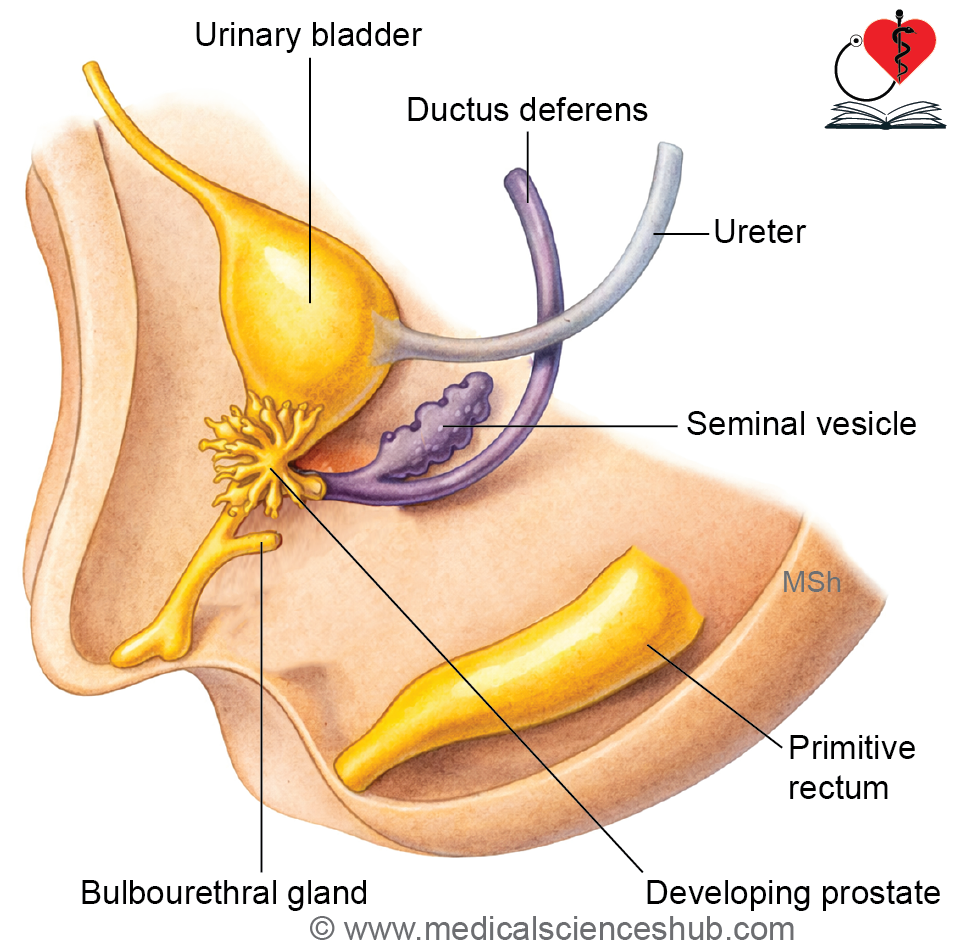
DEVELOPMENT OF PROSTATE
The prostate gland develops from both endodermal and mesodermal components associated with the prostatic urethra:
- Outer glandular zone:
Arises from epithelial buds that grow from the prostatic urethra (endoderm). - Inner glandular zone:
Develops from buds originating in the mesodermal posterior wall of the urethra, located above the openings of the ejaculatory ducts. Typically, five prostatic buds are formed: one anterior, two posterior, and two lateral. - Stroma (muscle, connective tissue, and capsule):
Derived from the surrounding mesoderm, which differentiates into the fibromuscular framework of the gland.
This coordinated interaction between endodermal epithelium and mesodermal stroma is essential for normal prostate formation.
DEVELOPMENT OF EXTERNAL GENITALIA
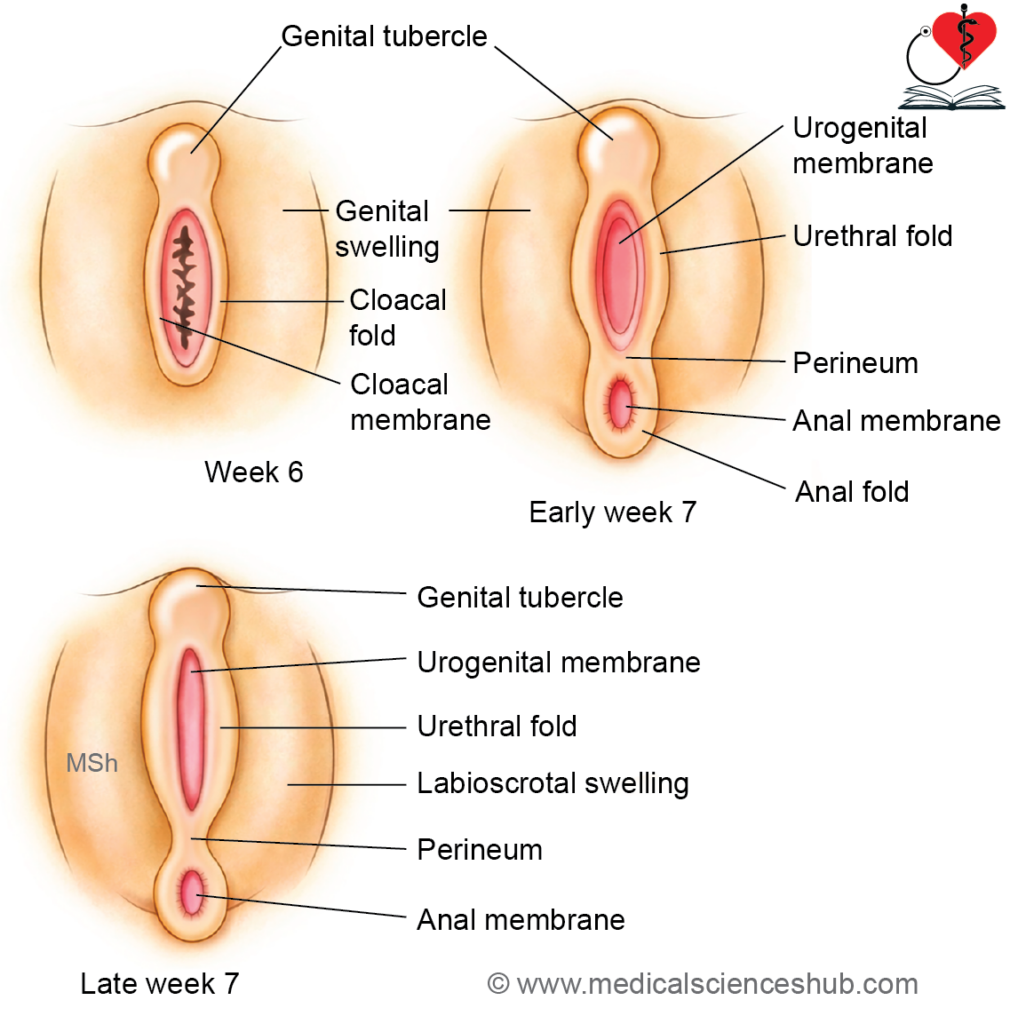
During early embryonic stages, the external genitalia of both sexes are morphologically identical. Differentiation begins around the 4th week:
- The somatopleuric lateral plate mesoderm proliferates around the cloacal membrane, forming raised structures called cloacal folds.
- The urorectal septum divides the cloacal membrane into a ventral urogenital membrane and a dorsal anal membrane. Simultaneously, the cloacal folds separate into urethral folds (anterior) and anal folds (posterior).
- On either side of the urethral folds, genital swellings appear, while a midline prominence forms the genital tubercle.
- The genital swellings develop into the scrotum in males and labia majora in females. The genital tubercle differentiates into the glans penis in males and the clitoris in females.
This early common pattern later undergoes sex-specific differentiation under hormonal influence.
Development of Male External Genitalia
Stages of Development
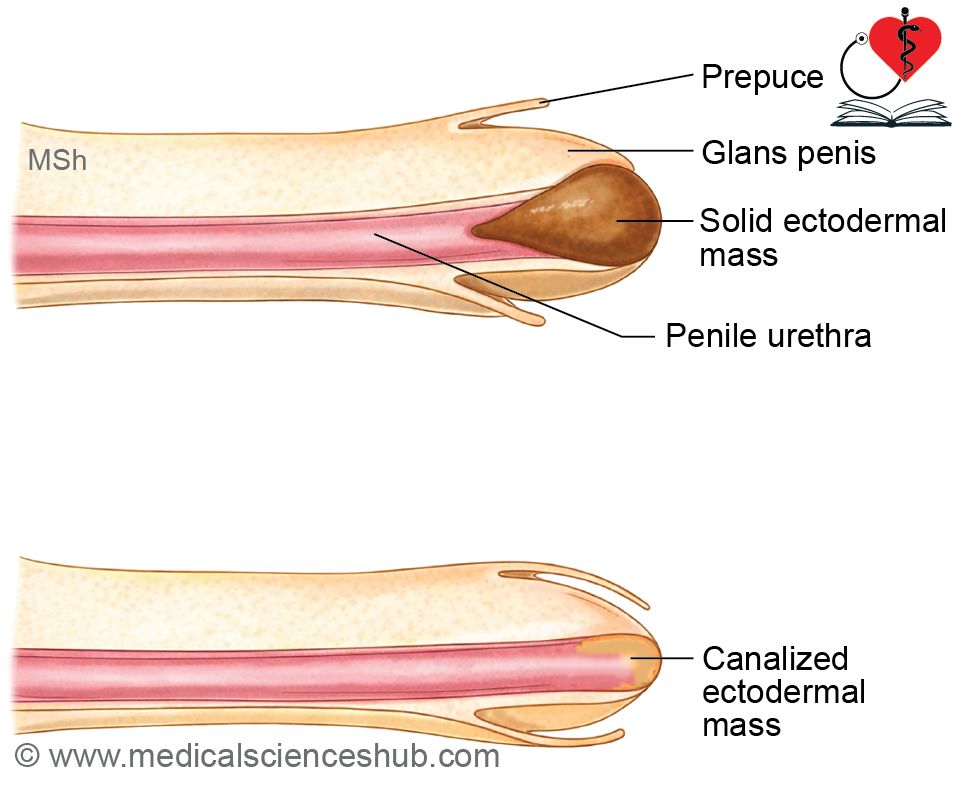
1. Formation of Penile Urethra
- The genital tubercle elongates to form the phallus (primitive penis). A urethral groove appears on its ventral surface and extends toward the tip.
- The endoderm of the phallic part of the urogenital sinus proliferates into the phallus, forming a solid urethral plate, which later canalizes to create the penile urethra.
- Rupture of the urogenital membrane deepens the groove into a definitive urethral groove, allowing communication with the exterior.
- The urethral folds fuse in a caudocranial direction to enclose the groove and form the urethra. The line of fusion is marked by the penile raphe.
- The terminal (glanular) part of the urethra develops from an ectodermal ingrowth, which subsequently canalizes.
2. Formation of Prepuce (Foreskin)
- A circular groove forms near the tip of the penis, separating the glans penis.
- Surrounding ectoderm proliferates to form the prepuce, which later covers the glans.
3. Formation of Scrotum
- The genital swellings enlarge to form scrotal swellings.
- These swellings fuse in the midline to form the scrotum, with the line of fusion indicated by the scrotal raphe.
Clinical Correlations
- Micropenis: Caused by inadequate androgen stimulation, often due to hypogonadism or hypothalamic–pituitary dysfunction.
- Bifid (double) penis: Results from splitting of the genital tubercle.
- Phimosis: A condition in which the prepuce is too narrow to retract over the glans.
This sequence highlights the coordinated roles of endoderm, ectoderm, and androgen-dependent differentiation in male genital development.
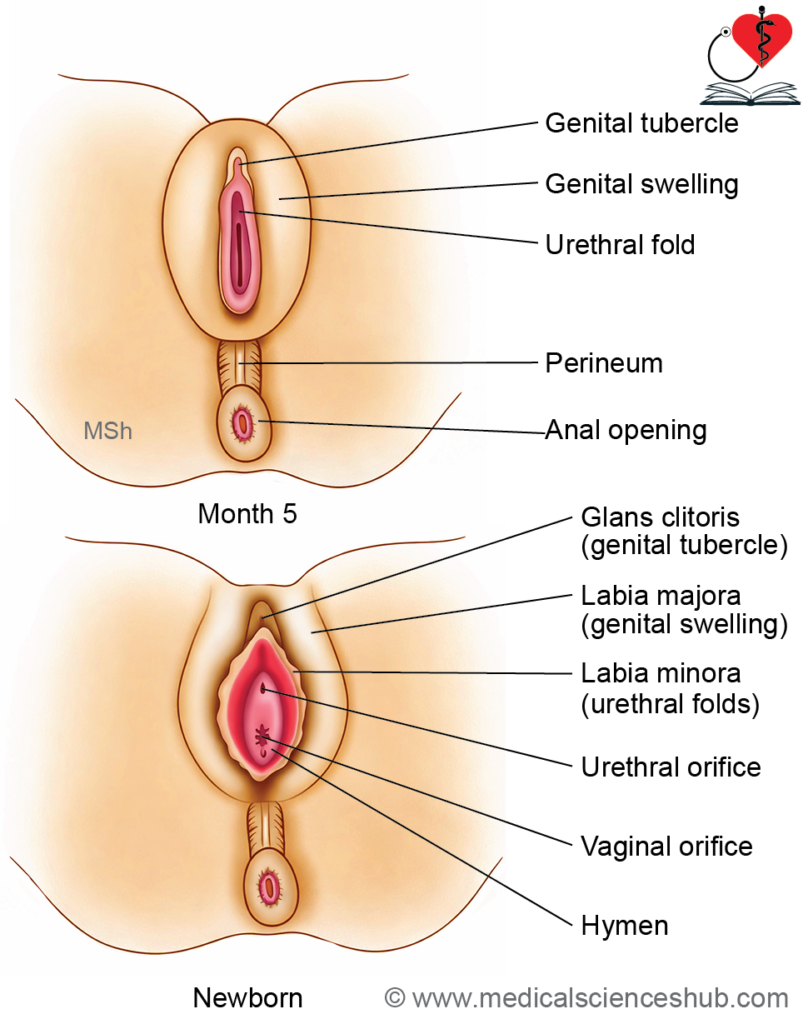
Development of Female External Genitalia
The female external genitalia develop from common embryonic structures under the influence of minimal androgen exposure:
- The genital tubercle elongates slightly to form the clitoris.
- The urethral folds remain unfused and give rise to the labia minora.
- The genital swellings enlarge to form the labia majora. These structures fuse posteriorly to form the posterior labial commissure, while anteriorly they contribute to the mons pubis and anterior labial commissure.
- The vestibule of the vagina is formed following rupture of the urogenital membrane, creating an opening into the urogenital sinus.
This pattern reflects the absence of fusion of urethral folds and the limited growth of the genital tubercle, which are key features of female differentiation.
CLINICAL EMBRYOLOGY
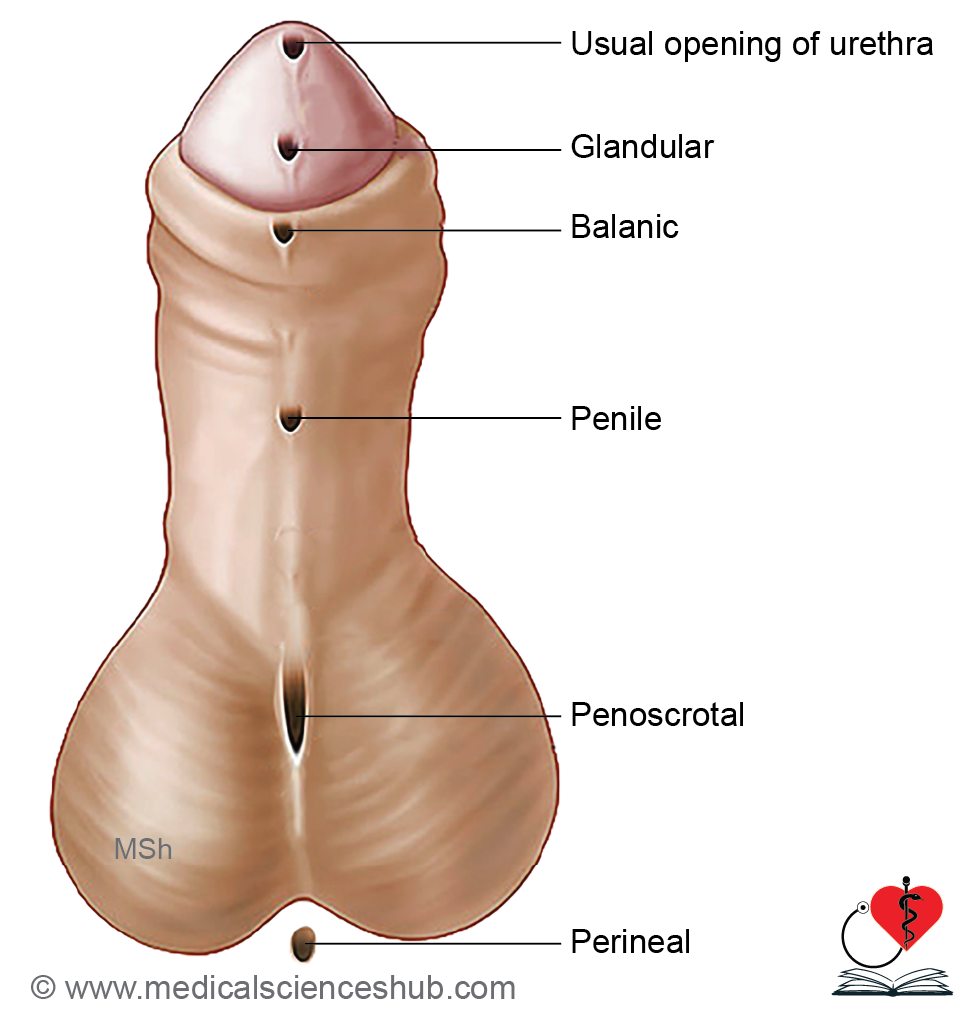
Hypospadias
Definition: A congenital urethral anomaly in which the external urethral meatus is located on the ventral surface of the penis rather than at its tip.
Incidence: Approximately 1 in 300 male births.
Embryological Basis:
- Failure of canalization of the ectodermal cord forming the terminal (glanular) urethra.
- Incomplete fusion of urethral folds, resulting in an open penile urethral groove.
Classification (based on meatal position):
- Glandular: Opening on ventral aspect of the glans.
- Balanic: Opening at the base of the glans.
- Penile: Opening along the ventral shaft of the penis.
- Penoscrotal: Opening at the junction of penis and scrotum.
- Perineal: Opening in the perineum due to failed fusion of labioscrotal folds.
Clinical Feature: Often associated with chordee, a downward curvature of the penis during erection.
Treatment: Definitive management is surgical correction.
Epispadias
Definition: A congenital anomaly in which the external urethral opening is located on the dorsal surface of the penis.
Incidence: Approximately 1 in 30,000 births.
Embryological Basis: The exact mechanism is uncertain; it is likely related to abnormal positioning or development of the genital tubercle.
Association: Commonly associated with bladder exstrophy (ectopia vesicae).Treatment: Managed by reconstructive surgery, often requiring a staged approach.
Important Questions
- Describe the embryological development of the testis.
- Explain the process of descent of the testis. Add a note on its clinical significance.
- Enumerate the factors that influence the descent of the testis.
- Write a short note on cryptorchidism, including its causes and clinical implications.
- Describe the embryological development of the ovary.
- Explain the development of the uterus, including the role of paramesonephric ducts.
- Write a short note on hypospadias, including its developmental basis and clinical features.
