Competencies
- AN78.5: Describe in brief abortion; decidual reaction, pregnancy test
- AN80.1: Describe formation, functions and fate of chorion, amnion, yolk sac, allantois, and decidua.
- AN80.2: Describe formation and structure of umbilical cord.
- AN80.3: Describe role of placenta, its physiological functions, foetomaternal circulation and placental barrier.
- AN80.5: Describe role of placental hormones in uterine growth and parturition.
- AN80.7: Describe various types of umbilical cord attachments.
INTRODUCTION
- From approximately the fifth month onward, the fetus swallows about 400 mL of amniotic fluid daily and excretes a similar volume of dilute urine into the amniotic cavity.
- The placenta is a temporary organ that enables exchange of oxygen, carbon dioxide, nutrients, and metabolic waste between the maternal and fetal circulations. It functions as a fetomaternal organ, supporting fetal growth and survival during pregnancy.
- It is a defining feature of eutherian (placental) mammals. The human placenta is discoid in shape and classified as choriodecidual, as it is formed from both fetal chorion and maternal decidua.
- The placenta consists of two main components:
- The maternal component, derived from the decidua basalis of the uterine endometrium.
- The fetal component, formed by the chorion frondosum, which develops from the trophoblast and extraembryonic mesoderm.
- After delivery of the fetus, the placenta and attached fetal membranes are normally expelled from the uterus during the third stage of labor, usually within 30 minutes.
Normal Attachment of Placenta
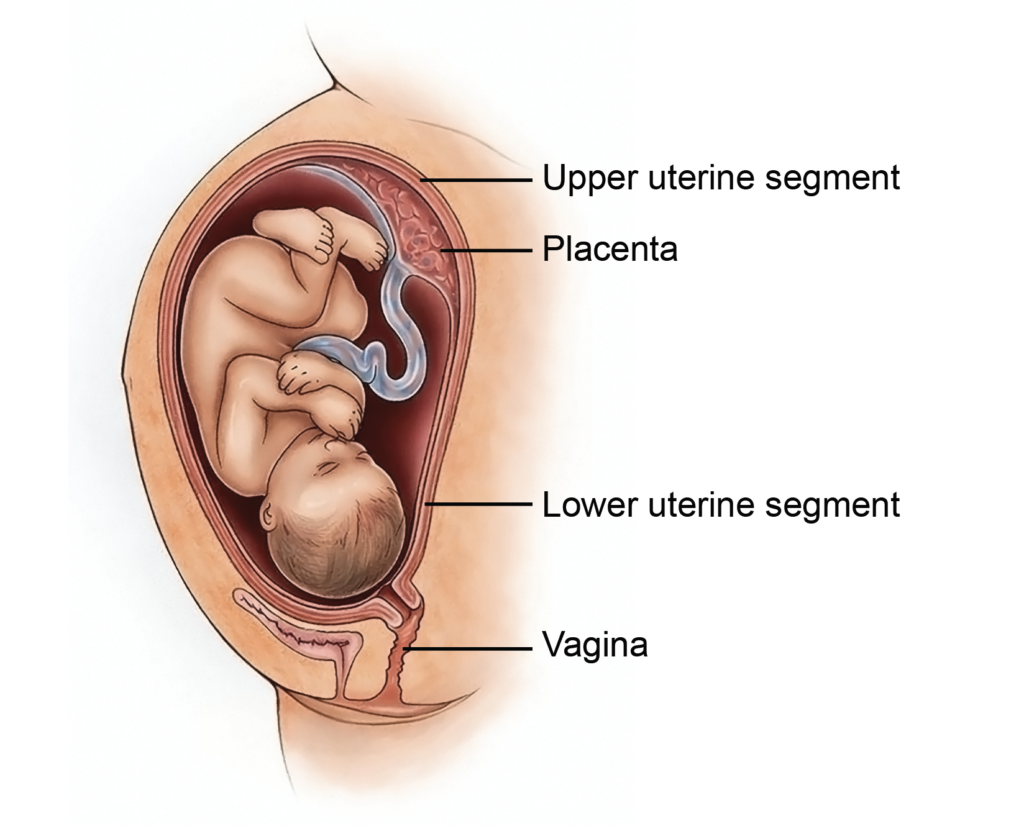
- The placenta normally implants in the upper segment of the uterus, most often along the posterior wall. This location supports adequate uterine blood flow and reduces the risk of bleeding during late pregnancy.
Gross Features
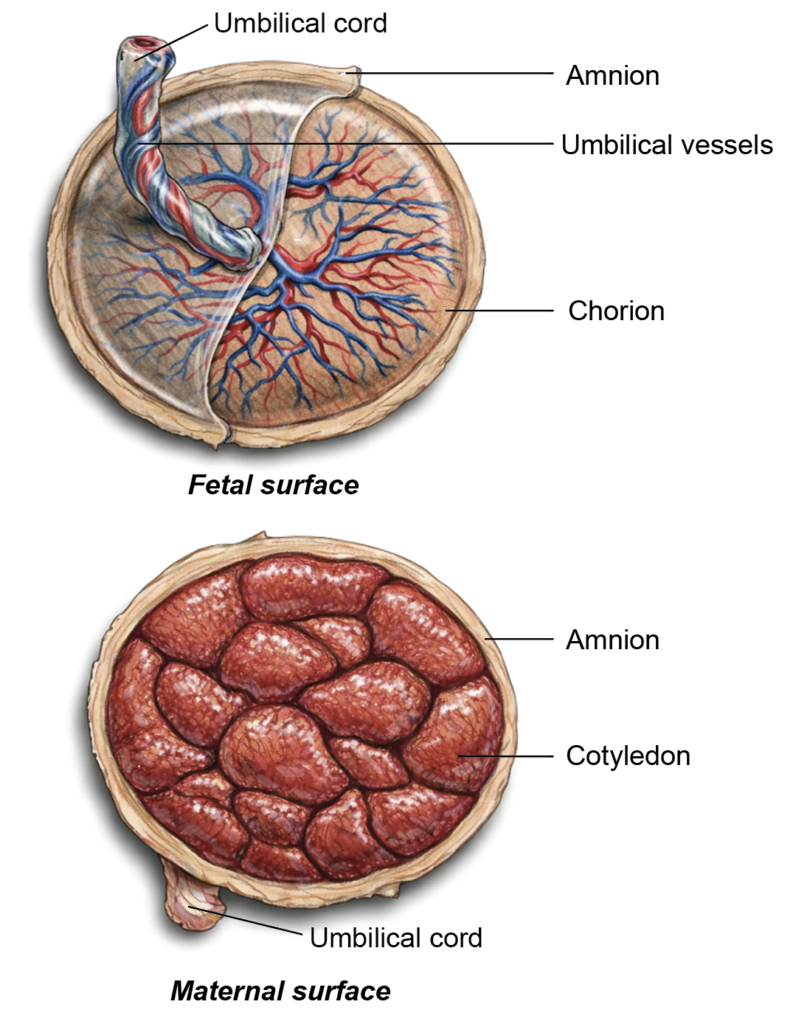
- At term, the placenta is a disc-shaped organ with two distinct surfaces: the maternal surface and the fetal surface.
Maternal Surface
- The maternal surface is rough and dark reddish-brown. It is divided into approximately 15–20 irregular, polygonal areas known as maternal cotyledons. These lobules are separated by grooves formed by decidual septa, producing a characteristic cobblestone pattern.
- Each maternal cotyledon generally contains one main stem villus and its branches, which participate in maternal–fetal exchange.
Fetal Surface
- The fetal surface is smooth, shiny, and greyish in appearance. It is covered by the amnion, which overlies the chorionic plate.
- The umbilical cord is attached to this surface, and the branching umbilical vessels can be seen radiating beneath the translucent amnion.
- The chorionic plate gives rise to 40–60 projections called fetal cotyledons, which extend toward the decidua basalis.
- Each fetal cotyledon consists of a stem villus and its subdivisions. One maternal cotyledon may correspond to one or more fetal cotyledons.
Measurements of the Full-Term Placenta
- At term (approximately 9 months of gestation), the placenta is typically discoid in shape.
- It measures about 15–25 cm in diameter and has an average central thickness of approximately 3 cm.
- The usual weight ranges from 500 to 600 grams.
- Placental growth occurs in proportion to the enlarging uterus and developing fetus. By term, the placenta occupies roughly 15–30% of the internal uterine surface, ensuring adequate area for maternal–fetal exchange.
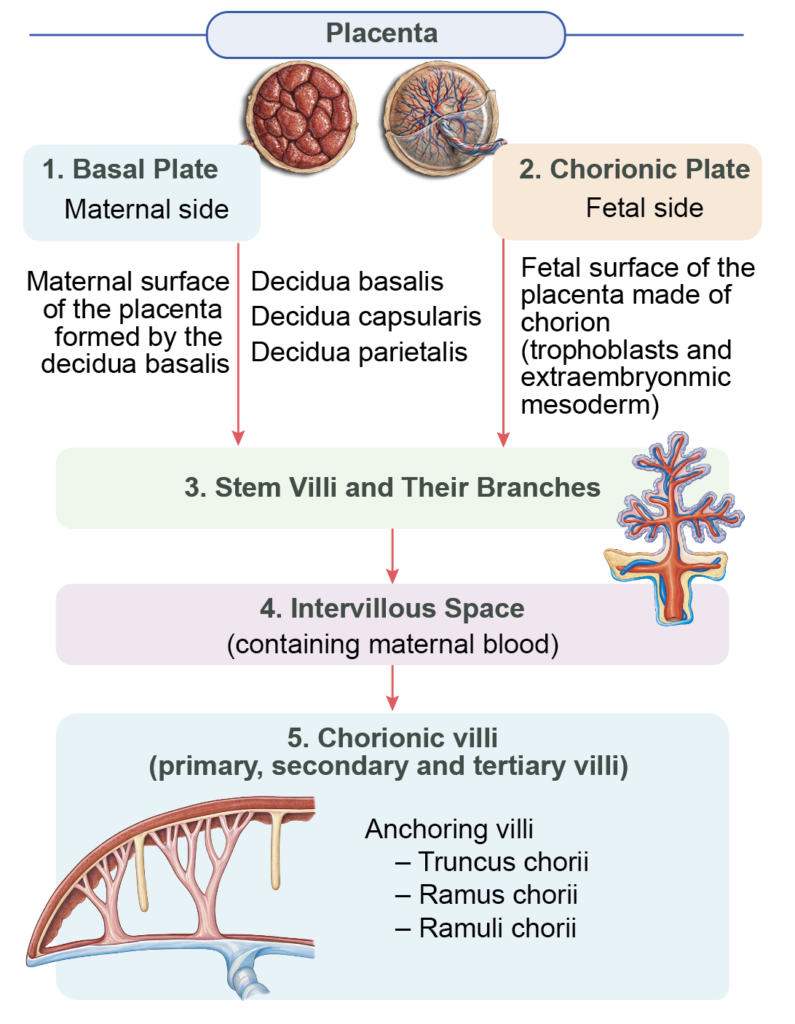
Structure of Placenta (Flowchart 9.1)
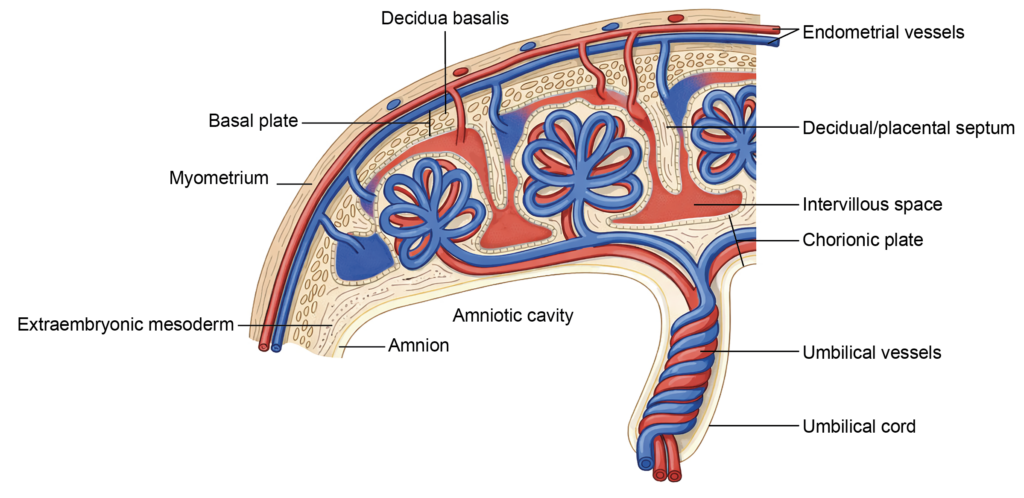
- The placenta is composed of four principal structural components:
- The basal plate on the maternal side
- The chorionic plate on the fetal side
- The stem villi and their branches
- The intervillous space containing maternal blood
- The basal and chorionic plates form the maternal and fetal boundaries of the placenta, respectively.
Basal Plate
- The basal plate constitutes the maternal surface of the placenta. It is formed by:
- The stratum spongiosum of the decidua basalis
- The cytotrophoblastic shell
- The overlying syncytiotrophoblast
- This region anchors the placenta to the uterine wall and supports maternal blood flow into the intervillous space.
Chorionic Plate
- The chorionic plate forms the fetal surface of the placenta.
- It consists of extraembryonic mesoderm, covered externally by cytotrophoblast and syncytiotrophoblast.
- From this plate arise the stem villi that extend into the intervillous space to facilitate maternal–fetal exchange.
Development of Placenta
Decidual Subdivisions
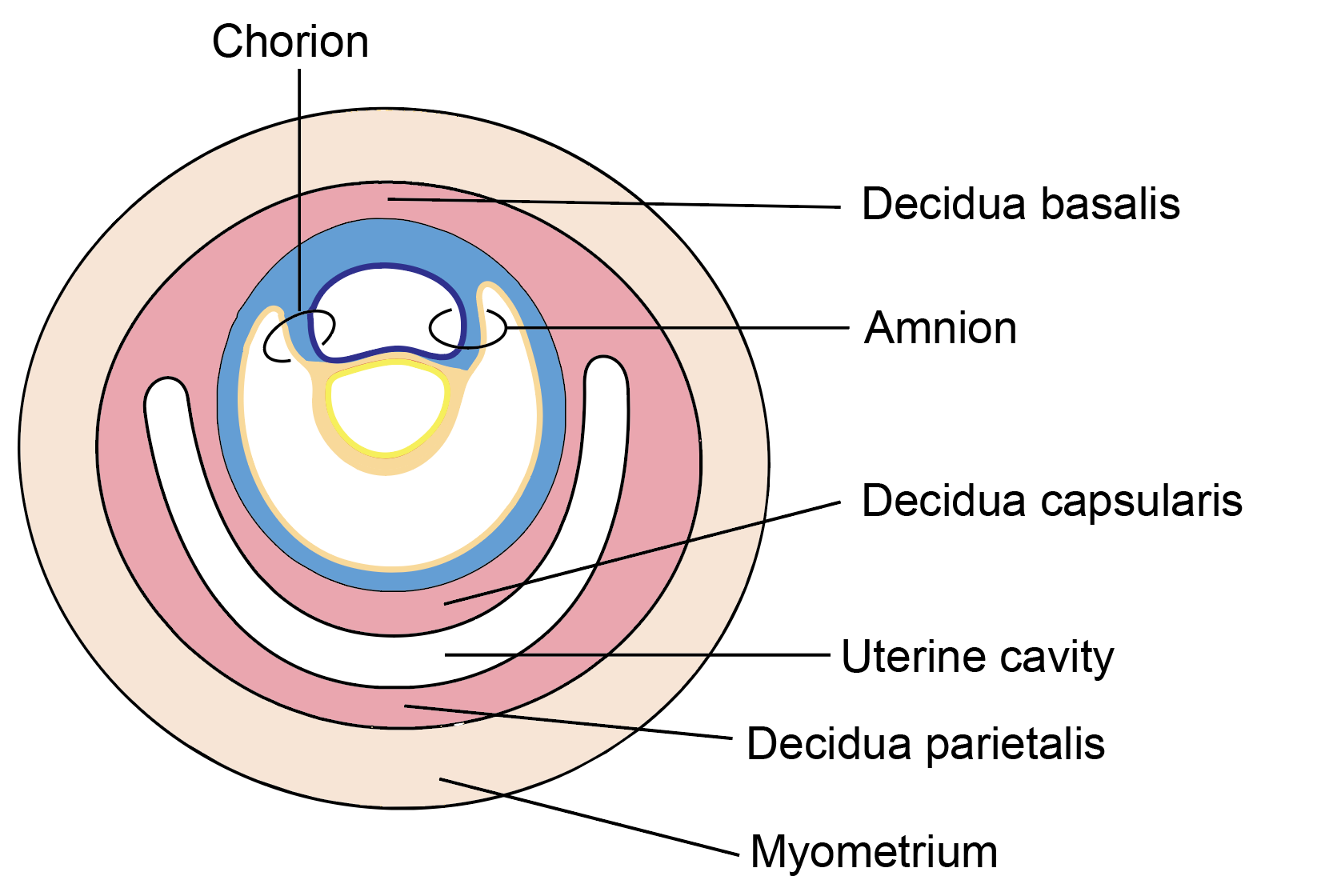
- During implantation, proliferating trophoblast invades the uterine endometrium, which undergoes decidual transformation. Once the blastocyst is fully embedded, the endometrium is divided into three regions:
- Decidua basalis, beneath the implantation site
- Decidua capsularis, covering the conceptus
- Decidua parietalis, lining the remainder of the uterine cavity
Formation of the Chorion
- The trophoblast differentiates into an outer syncytiotrophoblast and an inner cytotrophoblast.
- Cells derived from the epiblast form the extraembryonic mesoderm, which lines the trophoblast.
- Together, the syncytiotrophoblast, cytotrophoblast, and extraembryonic mesoderm constitute the chorion, the fetal membrane that contributes to placental development.
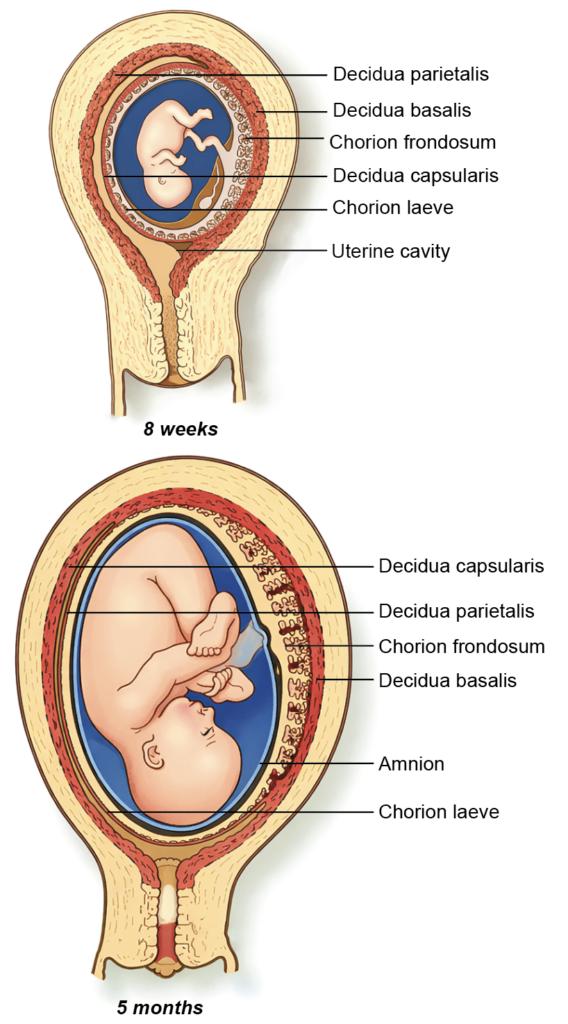
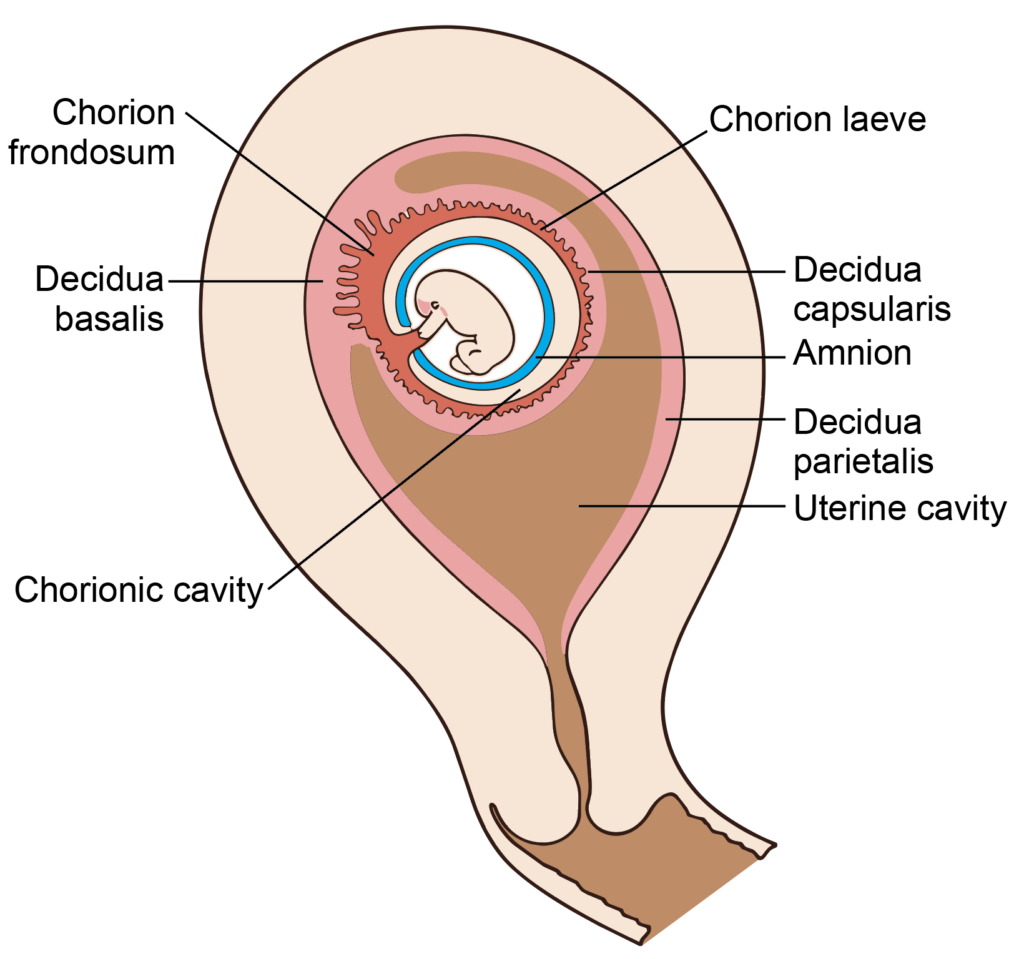
Figure 8.5a: Line diagram: Subdivisions of decidua, interstitial implantation (Click to see figure)
Uteroplacental Circulation
- Within the rapidly expanding syncytiotrophoblast, fluid-filled spaces called lacunae develop, particularly near the decidua basalis. These spaces enlarge and interconnect, while intervening syncytial columns form trabeculae.
- Progressive erosion of maternal capillaries allows maternal blood to enter the lacunae around days 17–22 of development, establishing the uteroplacental circulation.
Formation of Chorionic Villi
- Projections of syncytiotrophoblast are invaded by cytotrophoblast to form primary villi.
- Invasion of the villous core by extraembryonic mesoderm produces secondary villi.
- During the third week, formation of fetal capillaries within the mesoderm converts them into tertiary villi, capable of exchange. The surrounding lacunae are then termed intervillous spaces.
- Initially, villi surround the entire chorionic sac. Villi adjacent to the decidua capsularis regress, forming the smooth chorion laeve, whereas those near the decidua basalis proliferate extensively to create the chorion frondosum, which later forms the fetal part of the placenta.
Cytotrophoblastic Shell
- Cytotrophoblastic cells extend through the syncytiotrophoblast to form an outer cytotrophoblastic shell, anchoring the developing placenta to the maternal decidua.
Chorionic Villi and their Branching Pattern
- Chorionic villi develop in stages. Projections of syncytiotrophoblast are invaded by cytotrophoblast, forming primary villi.
- When extraembryonic mesoderm enters the core, they become secondary villi.
- With the development of fetal capillaries within the mesodermal core, they are termed tertiary villi, capable of exchange.
- Villi adjacent to the decidua basalis proliferate extensively to form the chorion frondosum, which constitutes the fetal part of the placenta.
- Villi related to the decidua capsularis regress, forming the smooth chorion laeve.
- Thus, the placenta is derived from the decidua basalis (maternal component) and the chorion frondosum (fetal component).
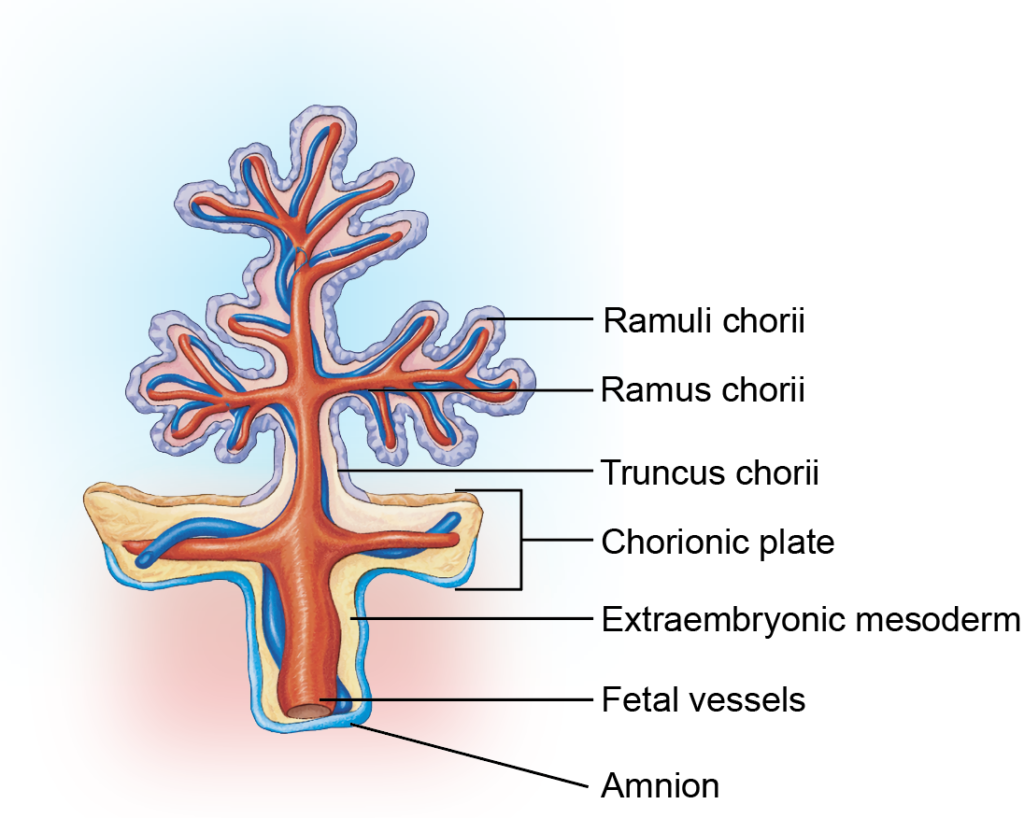
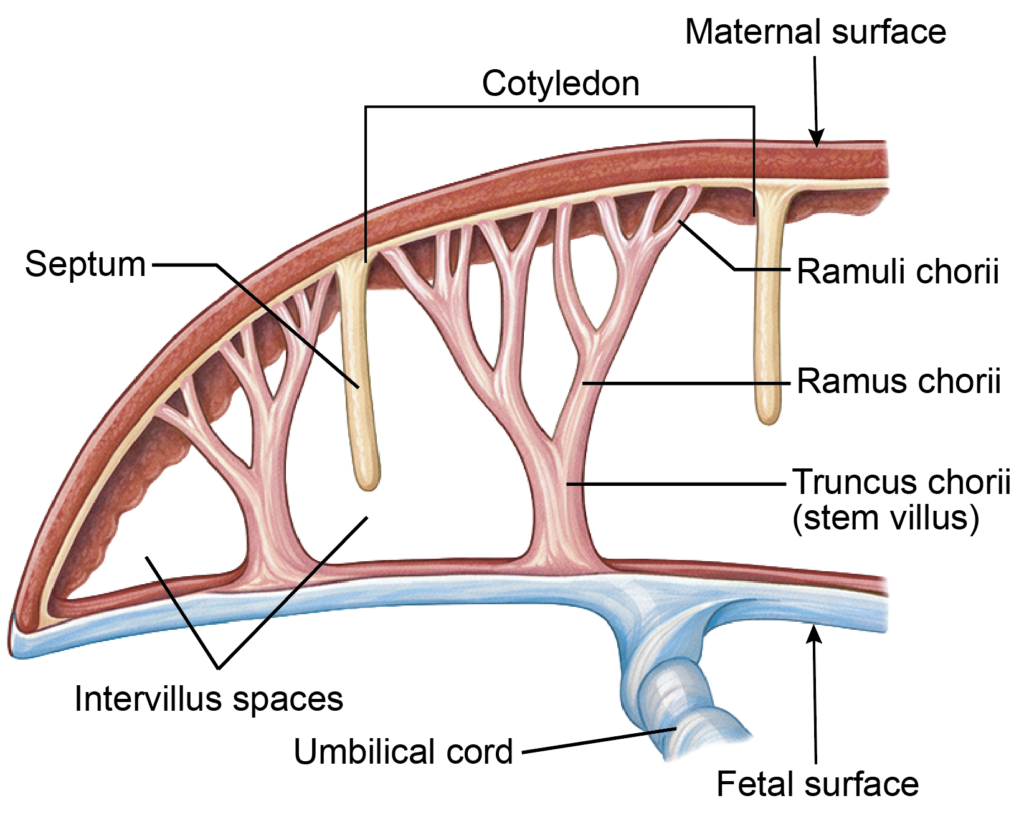
- Villi that extend from the chorion to the decidua basalis are known as anchoring villi. Their lateral branches project into the intervillous space and are classified as follows:
- Truncus chorii (stem villus): Connects the chorion to the decidua basalis
- Rami chorii: Primary branches of the stem villus
- Ramuli chorii: Smaller subdivisions of the rami
- Floating (free) villi: Numerous terminal villi suspended within the intervillous space
- The syncytiotrophoblast bears numerous microvilli that project into the intervillous space, markedly increasing the surface area for exchange, which may reach approximately 10–14 square meters at term.
- The tips of stem villi extend deepest into the decidua basalis, providing firm attachment of the placenta.
Placental Membrane or Barrier
- Within the placenta, maternal blood flows through the intervillous space, while fetal blood circulates in capillaries inside the chorionic villi.
- These two circulations remain separate and are divided by the placental membrane, which permits selective exchange without direct blood mixing.
- The placental membrane facilitates the transfer of oxygen, carbon dioxide, nutrients, electrolytes, antibodies, and fetal metabolic waste products.
Structure:
- In early pregnancy, the placental membrane measures approximately 20–25 µm in thickness and consists of:
- Endothelium of fetal capillaries
- Basement membrane of the fetal capillaries
- Extraembryonic mesoderm (villous stroma)
- Cytotrophoblast
- Syncytiotrophoblast
- From the fourth month onward, the cytotrophoblast largely disappears and the mesodermal layer becomes attenuated.
- As a result, the barrier is mainly formed by a thin syncytiotrophoblast layer and the fetal capillary endothelium.
- Near term, its thickness may reduce to approximately 2–5 µm, enhancing exchange efficiency.
- The total exchange surface area of the placental membrane at term ranges from 4 to 14 m², comparable to that of the adult intestinal mucosa.
Fibrinoid Layers of the Placenta
- Nitabuch’s layer refers to a zone of fibrinoid deposition located between the cytotrophoblastic shell and the decidua basalis. It forms a boundary between maternal and fetal tissues and contributes to controlled placental attachment.
- Rohr’s fibrinoid layer consists of fibrinoid material deposited on the surface of the syncytiotrophoblast facing the intervillous space. This layer is associated with trophoblastic remodeling and local regulation at the maternal–fetal interface.
- The cytotrophoblast is also known as the Langhans layer. It represents the inner cellular layer of the trophoblast beneath the syncytiotrophoblast. The term should not be confused with fibrinoid deposits, as it specifically denotes the cellular trophoblastic component.
- These structural specializations support placental stability and help maintain functional separation between maternal and fetal circulations.
Placental Changes at the End of Pregnancy
- As pregnancy approaches term, several structural and functional changes occur in the placenta:
- Progressive thinning of the placental membrane, which shortens the diffusion distance and facilitates gas exchange.
- Deposition of calcium salts (calcification), reflecting placental maturation and aging.
- Increased fibrosis and a reduction in effective villous surface area, which may limit exchange capacity.
- Decreased vascular density within some villi, reducing perfusion efficiency.
- Collectively, these changes may diminish the transfer of nutrients and waste products and slightly reduce hormonal production, including progesterone. In advanced or exaggerated cases, placental insufficiency may contribute to intrauterine growth restriction (IUGR).
Classification of Placenta (Flowchart 9.4)
According to Shape
- Based on gross morphology, the placenta is classified into the following types:
- Discoid placenta: A single, round or disc-shaped mass; this is the normal form in humans.
- Bidiscoid placenta: Composed of two nearly equal disc-shaped lobes connected by membranes.
- Lobed placenta (multilobed): Divided into two or more distinct lobes of variable size.
- Placenta succenturiata: Characterized by one or more small accessory lobes connected to the main placenta by blood vessels within the membranes.
- Placenta membranacea: The chorionic villi persist over most of the chorionic sac, producing a thin, diffuse placenta.
- Circum vallate placenta: The placental margin is raised and surrounded by a ring-like fold formed by inward reflection of the chorionic plate and decidua.
- These variations are clinically relevant, as some forms are associated with retained placental tissue or obstetric complications.
According to the Attachment of the Umbilical Cord
- Based on the site of insertion of the umbilical cord, the placenta is classified into the following types:
- Central insertion (normal placenta): The umbilical cord is attached near the center of the placental disc, providing balanced distribution of fetal vessels.
- Marginal insertion (battledore placenta): The cord is attached at or near the placental margin, resembling the shape of a badminton racquet.
- Velamentous insertion (velamentous placenta): The cord inserts into the fetal membranes close to the placental edge, and the umbilical vessels traverse between the amnion and chorion before reaching the placenta.
- Abnormal insertions, particularly velamentous insertion, are associated with increased risk of vessel compression or rupture.
According to Degree of Adhesion
- Based on the depth of abnormal attachment to the uterine wall, the placenta is classified as follows:
- Placenta accreta: The placental villi attach directly to the myometrium due to partial or complete absence of the decidua basalis, without deep invasion.
- Placenta increta: The villi invade into the myometrium.
- Placenta percreta: The villi penetrate through the entire uterine wall and may extend to adjacent structures, such as the urinary bladder.
- These conditions are collectively termed the placenta accreta spectrum (PAS) and are associated with a high risk of severe postpartum hemorrhage.
Functions of Placenta (Fig. 9.11)
- The placenta performs vital respiratory, nutritional, excretory, immunological, storage, and endocrine functions during pregnancy.
- Gaseous exchange: Oxygen (O₂) and carbon dioxide (CO₂) diffuse across the placental membrane. The high affinity of fetal hemoglobin for oxygen and its elevated concentration in fetal blood enhance oxygen transfer from mother to fetus.
- Nutrient transport: Essential nutrients such as glucose, amino acids, fatty acids, and electrolytes (sodium, potassium, chloride) are transferred through diffusion and active transport mechanisms.
- Excretion: Fetal waste products, including urea, uric acid, and creatinine, pass into maternal circulation for elimination.
- Passive immunity: Maternal IgG antibodies cross the placenta via receptor-mediated transport through the syncytiotrophoblast, providing temporary neonatal immunity. Protection depends on maternal antibody status and immunization history.
- Barrier function: The placenta restricts many bacteria and certain drugs; however, several viruses, toxins, and medications can cross. Limited passage of fetal cells into maternal blood may also occur.
- Storage: The placenta stores glycogen, iron, and calcium, supporting fetal growth.
- Endocrine function: The placenta acts as a temporary endocrine gland and secretes:
- Estrogens: Promote growth of the uterus, enlargement of the breasts, and relaxation of pelvic ligaments.
- Human chorionic gonadotropin (hCG): Structurally similar to luteinizing hormone (LH), it maintains the corpus luteum during early pregnancy (approximately the first trimester).
- Progesterone: Reduces myometrial contractility (progesterone block) and supports maintenance of the decidua.
- Human placental lactogen (hPL): Contributes to breast development and alters maternal metabolism to favor fetal nutrient supply
- Relaxin: Also produced by the corpus luteum, it promotes relaxation of pelvic ligaments and reduces uterine tone.
UMBILICAL CORD
- The umbilical cord is a flexible, tubular structure that connects the fetus to the placenta, enabling exchange between fetal and maternal circulations. It is covered externally by the amnion, which provides protection and a smooth surface.
The cord has two ends:
- The placental end, usually attached near the center of the placental disc.
- The fetal end, attached to the anterior abdominal wall at the umbilicus.
Measurements of Full-term Umbilical Cord
- At full term, the umbilical cord measures approximately 50–60 cm in length and about 2 cm in diameter. Its length allows adequate fetal movement while maintaining vascular continuity.
Development of Umbilical Cord
- During embryonic folding, part of the yolk sac and the connecting stalk are brought onto the ventral surface of the embryo.
- The junction between the amnion and surface ectoderm forms the umbilical ring, through which the vitelline (vitellointestinal) duct and allantois pass.
- The extraembryonic mesoderm within the connecting stalk becomes vascularized during the third and fourth weeks, forming two umbilical arteries and two umbilical veins.
- Later in development, the right umbilical vein regresses, leaving a single left umbilical vein.
- The surrounding mesenchymal tissue differentiates into a gelatinous connective tissue known as Wharton’s jelly, which protects the umbilical vessels from compression.
Contents of Umbilical Cord
The umbilical cord contains the following structures:
1. Umbilical vessels:
- At term, the cord contains two umbilical arteries and one umbilical vein.
- The arteries arise from the fetal internal iliac arteries and carry deoxygenated blood to the placenta.
- Initially, two umbilical veins are present, but the right umbilical vein regresses early in development.
- The persistent left umbilical vein transports oxygenated blood from the placenta to the fetus.
- It joins the left branch of the portal vein, and most of this blood reaches the inferior vena cava through the ductus venosus.
2. Wharton’s jelly: This is a specialized mucoid connective tissue derived from extraembryonic mesoderm.
- It surrounds and protects the umbilical vessels from compression.
- Coiling of the vessels within this tissue gives the cord its characteristic spiral appearance.
3. Allantoic remnant: A portion of the allantois extends into the cord during early development. Its intra-abdominal part later forms the urachus, while the remaining portion contributes to the urinary bladder.
4. Vitelline duct remnants: The vitelline (vitellointestinal) duct, which connects the midgut to the yolk sac, and residual parts of the yolk sac (sometimes termed the umbilical vesicle) may be present early in development. These structures normally degenerate as pregnancy progresses.
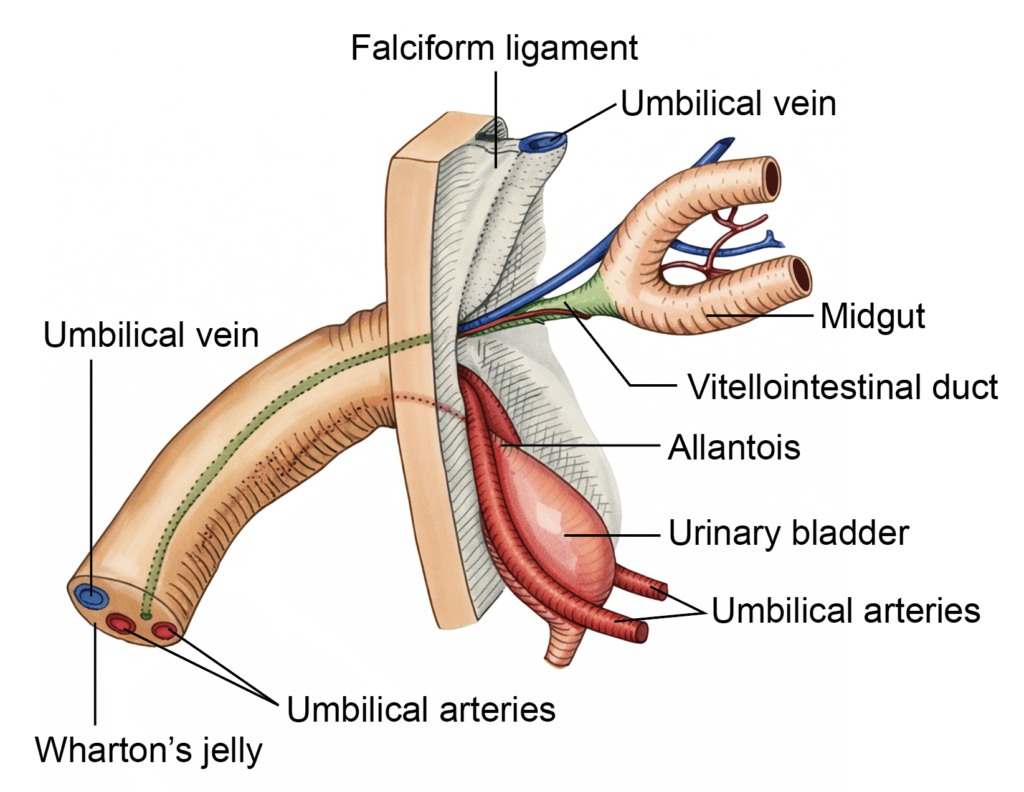
Figure 8.9a: Line diagram: Structure of the umbilical cord (Click to see figure)

CLINICAL EMBRYOLOGY
- Common Anomalies of the Umbilical Cord
- Single Umbilical Artery:In this anomaly, only one umbilical artery is present instead of the usual two. It occurs in approximately 1 in 200 live births. This finding is frequently associated with congenital cardiac defects and other vascular or systemic malformations.
- True Knot of the Umbilical Cord:A true knot forms when the cord loops upon itself and tightens, which may compromise fetoplacental blood flow, particularly during labor. In contrast, a false knot represents a localized bulge caused by redundancy or tortuosity of umbilical vessels and has no clinical significance.
- Nuchal Cord:A nuchal cord occurs when the umbilical cord encircles the fetal neck. While often asymptomatic, tight looping may intermittently reduce blood flow during uterine contractions.
- Cord Prolapse:Umbilical cord prolapse refers to descent of the cord into the birth canal ahead of the presenting fetal part. This condition can result in cord compression and reduced fetal oxygenation, requiring urgent obstetric management.
- Velamentous Insertion:In velamentous cord insertion, the umbilical vessels traverse the fetal membranes before reaching the placenta, rather than inserting directly into placental tissue. These exposed vessels are vulnerable to rupture, particularly during membrane rupture or labor.
AMNION
- The amnion is a thin, transparent fetal membrane that forms the roof of the amniotic cavity and surrounds the developing embryo.
- During the second week of development, cells from the embryoblast differentiate into amnioblasts, which line the newly formed amniotic cavity. The amnion forms the roof of this cavity, while the bilaminar germ disc constitutes its floor. Structurally, the amnion consists of a layer of amniotic epithelium supported by extraembryonic somatic mesoderm (somatopleuric mesoderm).
- By the end of the eighth week, as a result of embryonic folding and expansion of the amniotic cavity, the amnion completely encloses the embryo. The cavity contains amniotic fluid (liquor amnii), which provides cushioning and permits fetal movements.
Constituents of Amniotic Fluid
Amniotic fluid is a clear, pale fluid that fills the amniotic cavity and surrounds the fetus. Its composition changes with gestational age. The principal components include:
- Water (approximately 98–99%) and dissolved electrolytes.
- Fetal urine and small amounts of other fetal metabolic waste products.
- Trace quantities of hormones, including human chorionic gonadotropin (hCG) and human placental lactogen (hPL).
- Exfoliated fetal cells, derived mainly from the skin, respiratory tract, and urinary tract.
These constituents reflect continuous exchange between the fetus, placenta, and maternal circulation.
Functions of Amniotic Fluid
Amniotic fluid performs several essential roles during fetal development:
- Shock absorption: It acts as a protective fluid cushion, reducing the impact of external mechanical forces and minimizing injury to the fetus.
- Support of development: In early stages, it facilitates normal growth of surface structures, including closure of the neuropores, by preventing adhesion and allowing expansion of developing tissues.
- Facilitation of movement: The fluid permits free fetal movements, which are important for musculoskeletal development and joint formation.
- Fluid exchange and waste removal: The fetus releases urine into the amniotic cavity and also swallows amniotic fluid. Absorbed fluid enters the fetal circulation, and metabolic waste products are transferred to the maternal blood through the fetoplacental circulation.
Volume of Amniotic Fluid
- The volume of amniotic fluid progressively increases from the 10th to the 28th week of gestation, reaching a peak during the third trimester. After this period, the volume gradually declines toward term.
- This dynamic balance between swallowing and urination maintains fluid volume.
- Fetal metabolic waste products are transferred to the maternal circulation through the placenta.
Amniotic Fluid Volume at Different Stages of Pregnancy
| Gestational Age | Approximate Mean Volume | Physiological Features and Mechanisms |
|---|---|---|
| 10 weeks | 25–30 mL | The amniotic cavity contains a small amount of fluid, primarily derived from maternal plasma diffusion across the fetal membranes and early secretory activity of the amnion. |
| 20 weeks | 350–500 mL | The volume rises steadily due to increasing fetal urine production and fluid exchange across the membranes. The onset of consistent fetal swallowing contributes to regulation of fluid balance. |
| 28 weeks | 700–1,000 mL | Rapid fetal growth is associated with active renal function. A dynamic equilibrium develops between urination and swallowing, maintaining relative stability of fluid volume. |
| 34–36 weeks | 800–1,000 mL (maximum) | The volume reaches its peak during the late third trimester. Thereafter, a gradual physiological decline begins as placental transfer and fetal maturation alter fluid dynamics. |
| 40 weeks (term) | 700–800 mL | At term, the volume is slightly reduced but remains adequate to provide mechanical cushioning and allow normal fetal movement. |
| 42 weeks (post-term) | 300–500 mL | In prolonged pregnancy, further reduction may occur, increasing the likelihood of oligohydramnios due to reduced placental efficiency and diminished fetal urine output. |
CLINICAL EMBRYOLOGY
- Clinical Conditions Related to Amniotic Fluid and Membranes
- Amniocentesis: Itis an invasive diagnostic procedure in which approximately 20–30 mL of amniotic fluid is aspirated under ultrasound guidance. The sample is analyzed for biochemical markers, such as the lecithin–sphingomyelin (L:S) ratio to assess fetal lung maturity, and for chromosomal abnormalities using karyotyping or molecular techniques. Elevated alpha-fetoprotein (AFP) levels may indicate neural tube defects.
- Oligohydramnios: It refers to reduced amniotic fluid volume, typically less than 400–500 mL at term. On ultrasonography, it is suggested when the single deepest vertical pocket measures less than 2 cm or when the amniotic fluid index (AFI) is below 5 cm.
- Amnion Nodosum:It consists of small nodular lesions on the fetal surface of the amnion, commonly associated with oligohydramnios. These nodules are formed by aggregates of squamous epithelial cells derived from vernix caseosa.
- Potter Sequence: It results from severe oligohydramnios and is characterized by pulmonary hypoplasia, limb deformities, characteristic facial features, and frequently renal agenesis. Causes include fetal renal anomalies, chronic leakage of amniotic fluid, or placental insufficiency.
- Polyhydramnios: It denotes excessive amniotic fluid, generally exceeding 2,000 mL at term. It is diagnosed when the AFI exceeds 24 cm. Common causes include impaired fetal swallowing, as seen in esophageal atresia, and central nervous system anomalies such as anencephaly.
- Amniotic Band Syndrome: It is a rare disorder caused by fibrous strands from the ruptured amnion that entangle fetal parts. These bands may produce constriction rings, limb deformities, or even intrauterine amputation. Craniofacial abnormalities may also occur.
- Premature Rupture of Membranes (PROM):
- PROM refers to rupture of the fetal membranes before the onset of labor at or after 37 weeks of gestation. When membrane rupture occurs before 37 weeks, it is termed preterm premature rupture of membranes (PPROM) and is associated with increased risk of preterm birth and infection.
CLINICAL EMBRYOLOGY
- Placenta Previa
- It is defined as implantation of the placenta in the lower uterine segment, such that it partially or completely overlies the internal cervical os. The term “previa” means “situated before,” indicating that the placenta lies in front of the presenting fetal part at the cervical opening.
- Incidence: Placenta previa occurs in approximately 0.5–1% of hospital deliveries. Its frequency increases with advancing maternal age, particularly in women older than 35 years. Other recognized risk factors include multiparity, previous cesarean section, and prior uterine surgery.
- Classification: Placenta previa is classified according to the relationship of the placental edge to the internal os:
- Type I (Low-lying placenta): The placenta is located in the lower uterine segment but does not reach the internal os.
- Type II (Marginal placenta previa): The placental margin reaches the edge of the internal os but does not cover it.
- Type III (Partial placenta previa): The placenta partially covers the internal os.
- Type IV (Complete placenta previa): The placenta completely covers the internal os.
- Types I and II are considered minor placenta previa, whereas Types III and IV are classified as major placenta previa because they are more likely to cause significant bleeding and usually require cesarean delivery.
- Diagnosis
- Ultrasonography, particularly transvaginal ultrasound in the third trimester, is the most accurate and safe method for diagnosing placenta previa. It precisely determines the placental location and its relation to the internal os.
- Complications
- Placenta previa is a major cause of antepartum hemorrhage, defined as bleeding from the genital tract after 28 weeks of gestation and before delivery. The bleeding is typically painless and may recur. Severe cases can lead to maternal anemia, fetal distress, preterm birth, and increased perinatal morbidity.
Important Questions
- Describe the placenta, detailing its gross structure. Include a clearly labeled diagram showing both the maternal surface and the fetal surface.
- Explain the intervillous space of the placenta, outlining its development, anatomical boundaries, contents, and functional importance in maternofetal exchange.
- Discuss the chorionic villi, including their stages of development, microscopic structure, and role in placental function.
- Describe the placental barrier, listing its structural components and explaining its role in selective transfer between maternal and fetal circulations.
- Classify the placenta according to its shape and distribution of chorionic villi, and briefly describe each type.
- Enumerate and explain the major functions of the placenta, including its roles in exchange, protection, and metabolism.
- Outline the endocrine functions of the placenta. List the principal hormones it secretes and describe their physiological effects during pregnancy.
- Write a short note on placenta previa, discussing its anatomical basis and clinical implications.
- Describe the umbilical cord, including its embryological development and structural characteristics.
- List the anatomical contents of the umbilical cord.
- Describe the yolk sac, outlining its development and its functions during early embryonic life.
