Competencies
- AN52.7: Describe the development of urinary system.
INTRODUCTION
- The urinary and genital systems develop from two common embryonic sources: the intermediate mesoderm and the cloaca. These structures provide the foundational tissues from which the organs of the genitourinary system arise.
Intermediate Mesoderm
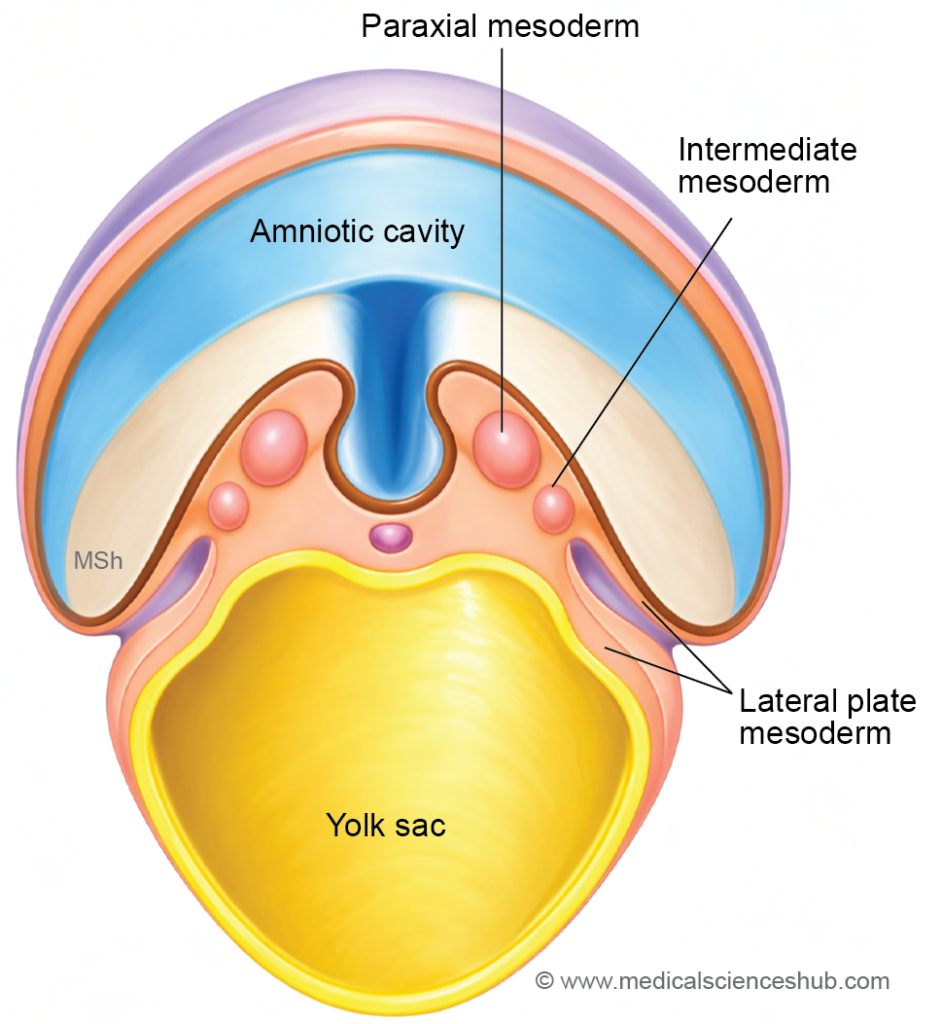
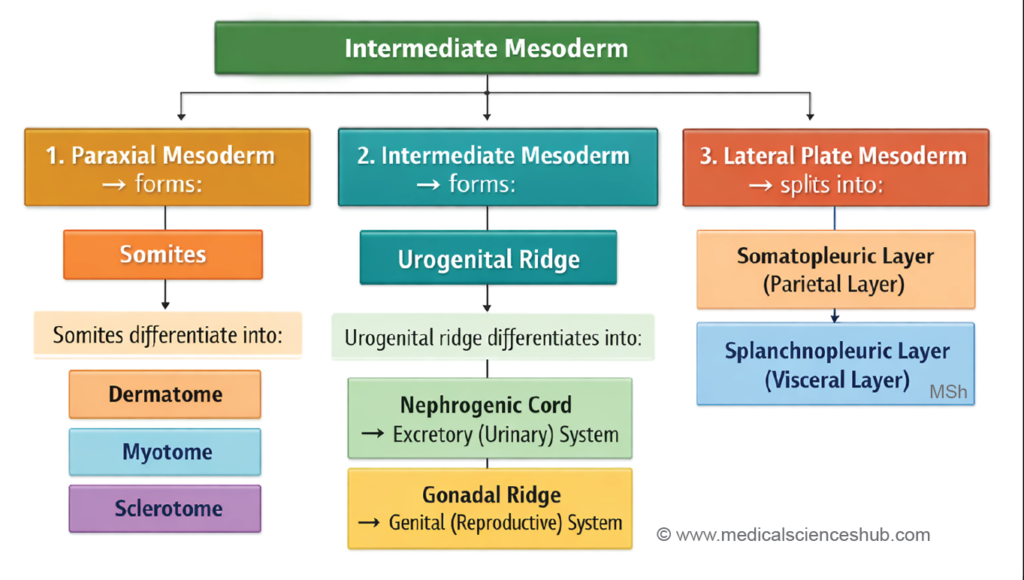
- During early embryonic development, the intraembryonic mesoderm differentiates into three longitudinal regions after the formation of somites and the intraembryonic coelom:
- Paraxial mesoderm, which gives rise to somites.
- Intermediate mesoderm, which forms most components of the genitourinary system.
- Lateral plate mesoderm, which divides into somatopleuric and splanchnopleuric layers.
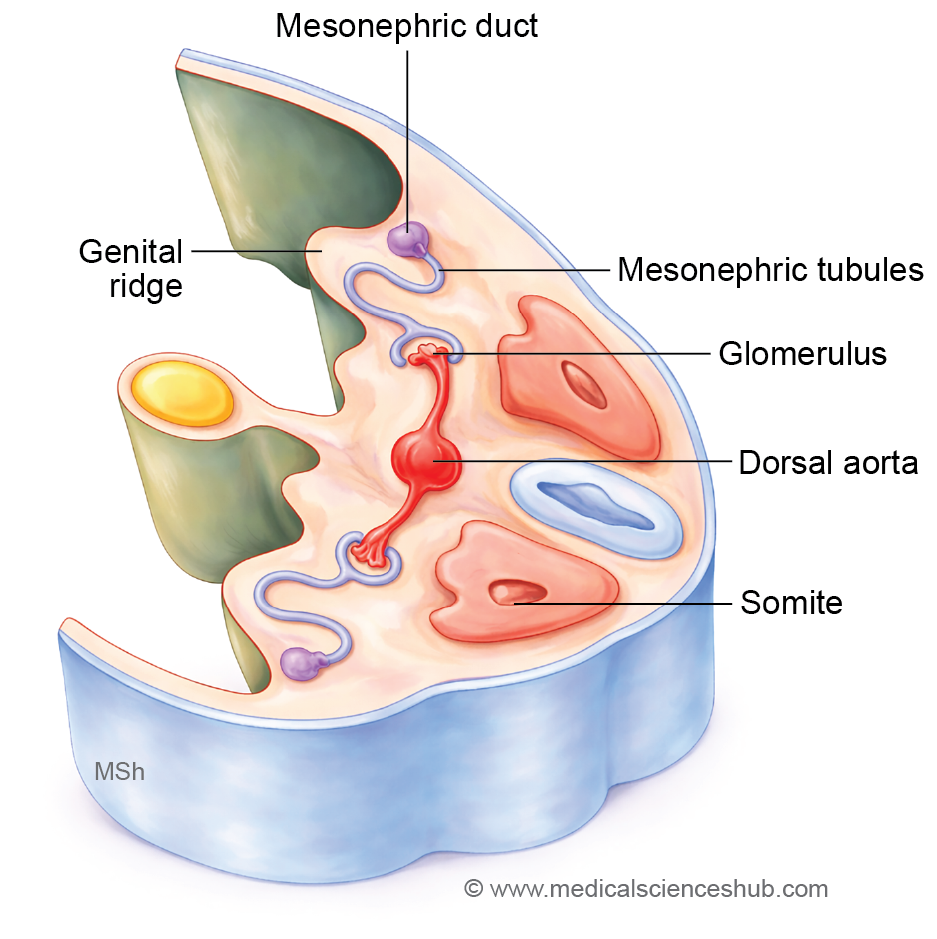
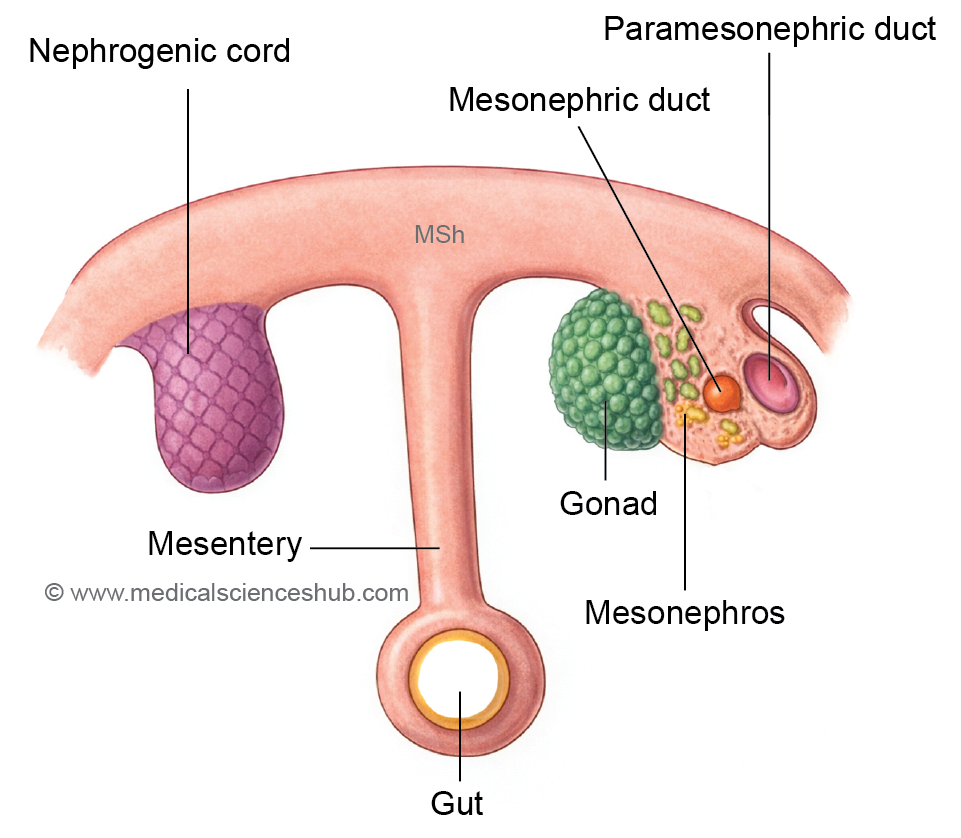
- The intermediate mesoderm forms a longitudinal elevation called the urogenital ridge along the dorsal body wall, situated lateral to the attachment of the dorsal mesentery. This ridge differentiates into two distinct parts:
- the genital ridge (medial part), which contributes to the developing gonads, and
- the nephrogenic cord (lateral part).
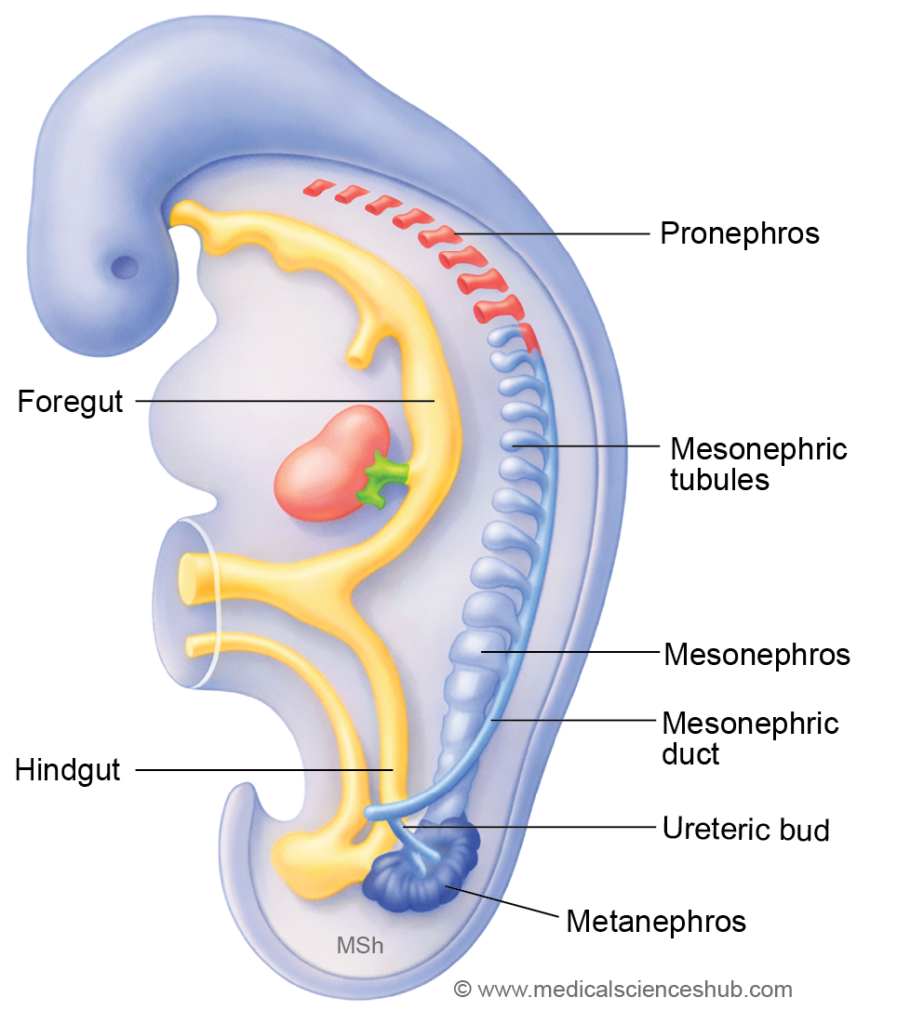
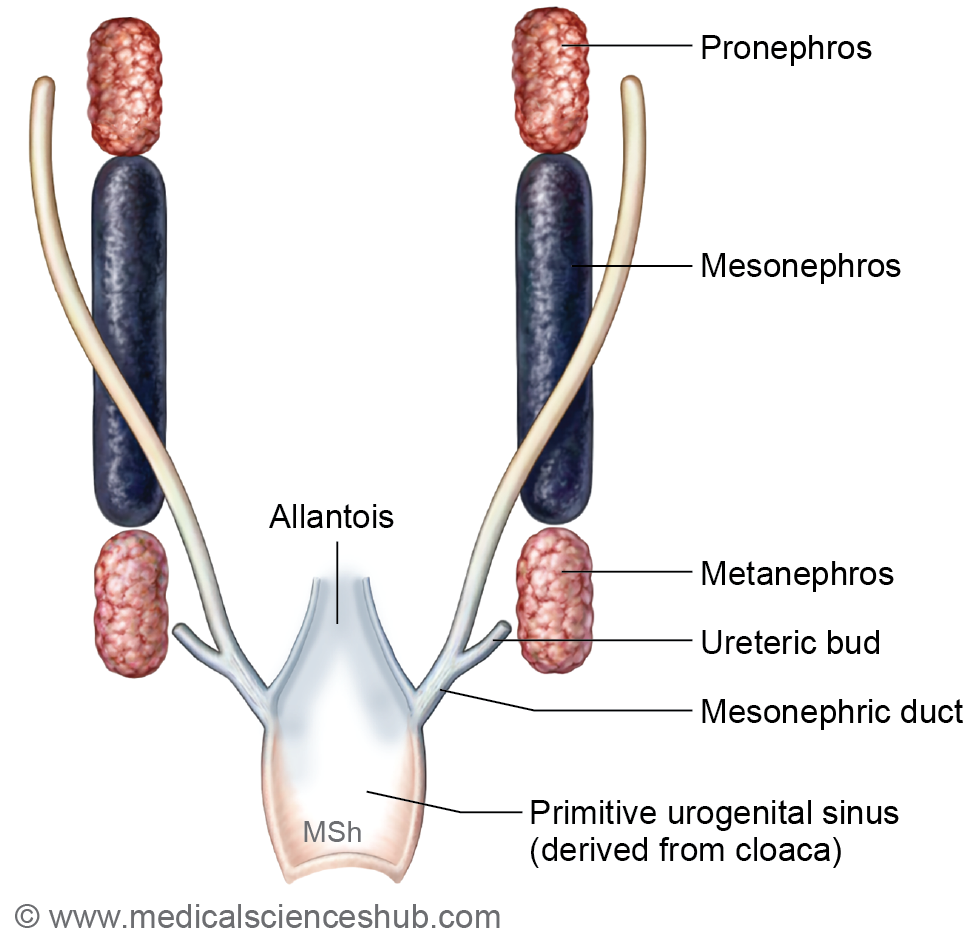
- The nephrogenic cord extends from the cervical to sacral regions of the embryo. During development, it progresses through three successive stages—pronephros, mesonephros, and metanephros—which are associated with the formation of renal tubules, the mesonephric ducts, the paramesonephric ducts, and related structures of the urinary and reproductive systems.
Cloaca
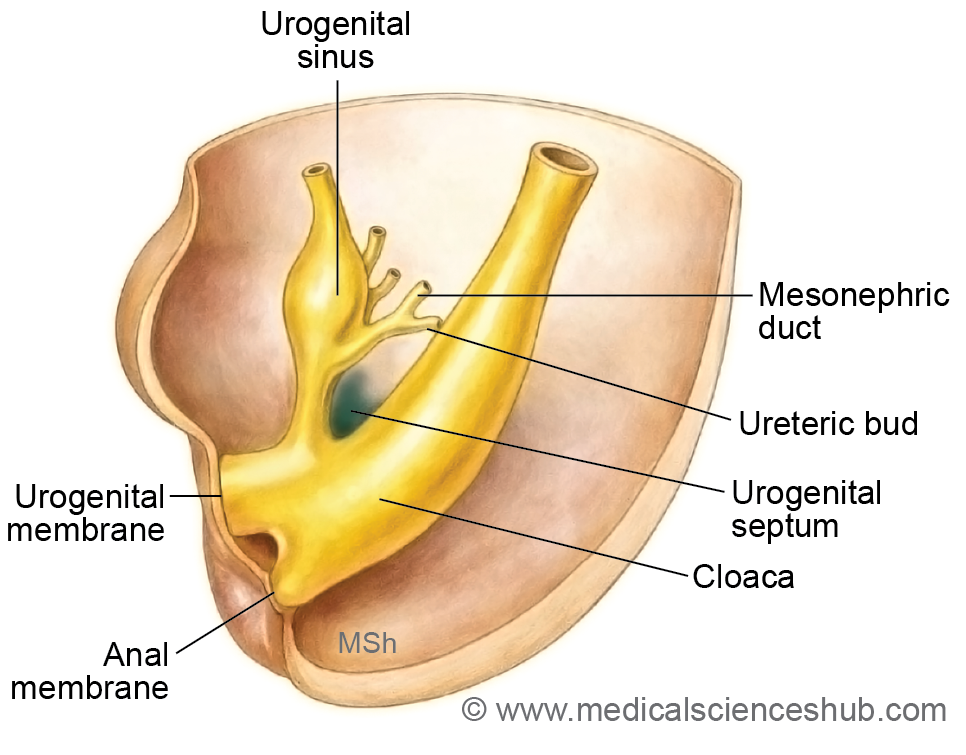
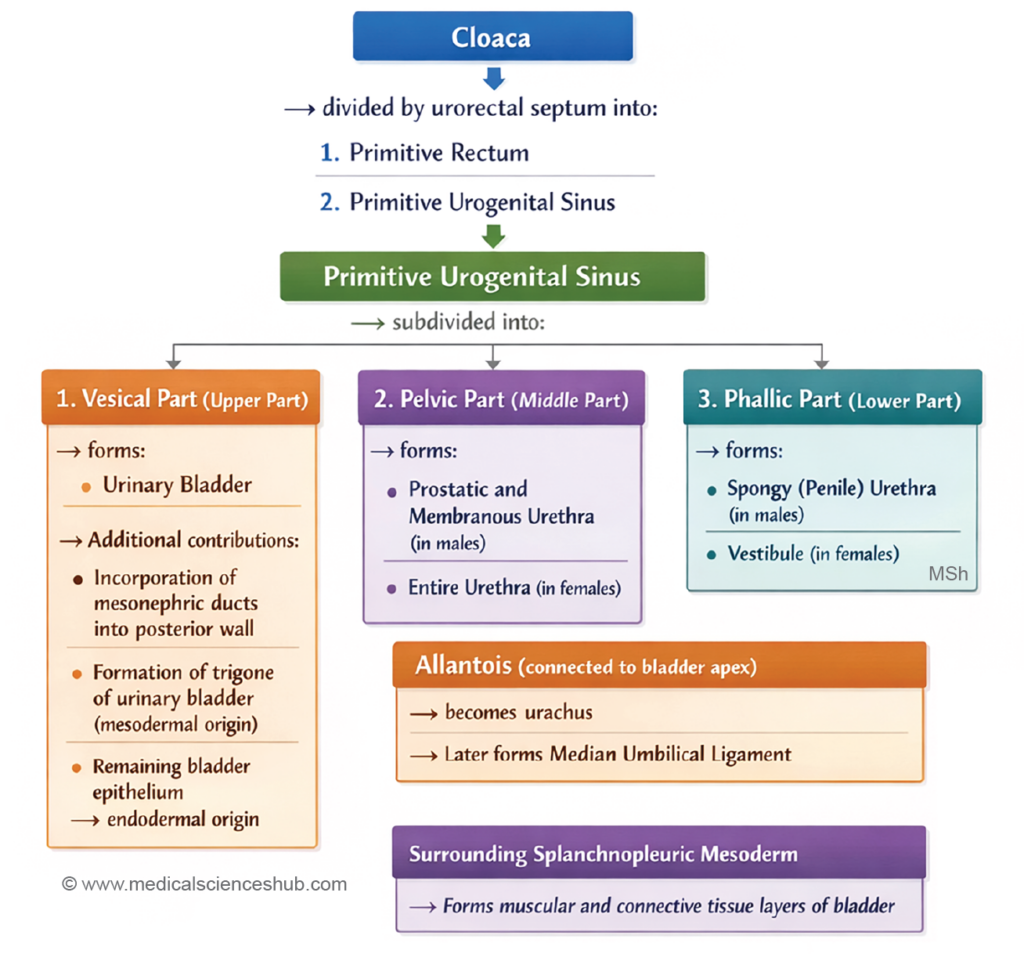
- The cloaca represents the terminal part of the hindgut and initially serves as a common cavity for both the digestive and genitourinary systems. It is subsequently divided by the urorectal septum into two regions:
- the primitive urogenital sinus anteriorly, and
- the primitive rectum posteriorly.
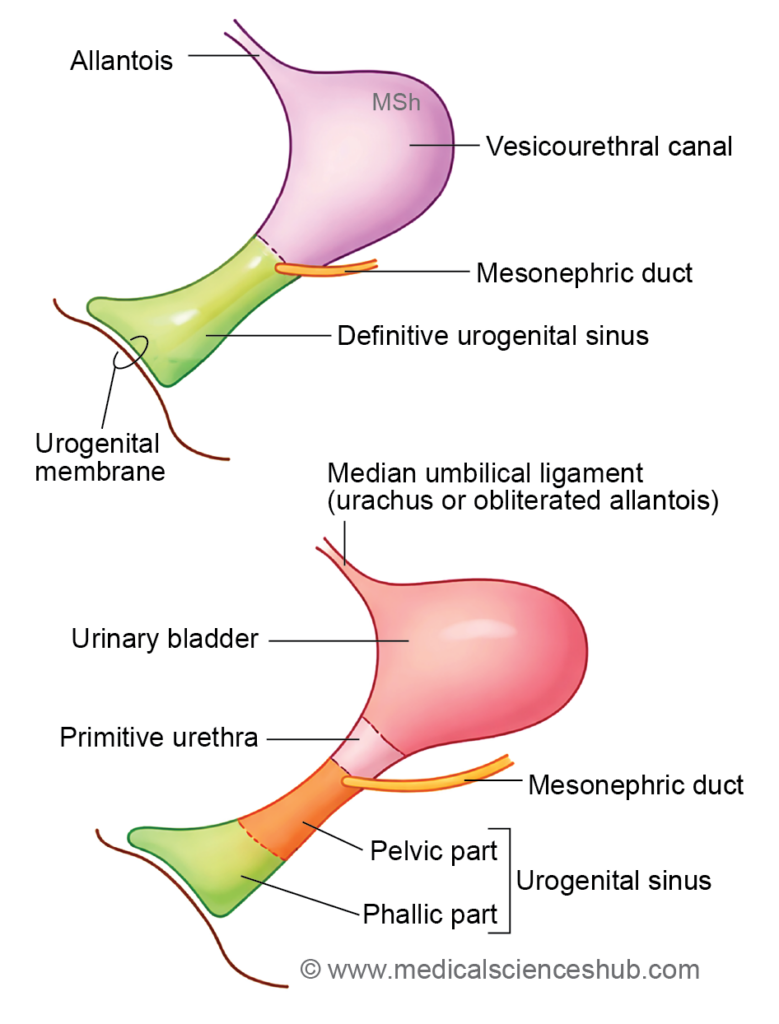
- Later, the entry of the mesonephric ducts further subdivides the primitive urogenital sinus into a cranial vesicourethral canal and a caudal definitive urogenital sinus, which contribute to the formation of parts of the urinary bladder and urethra.
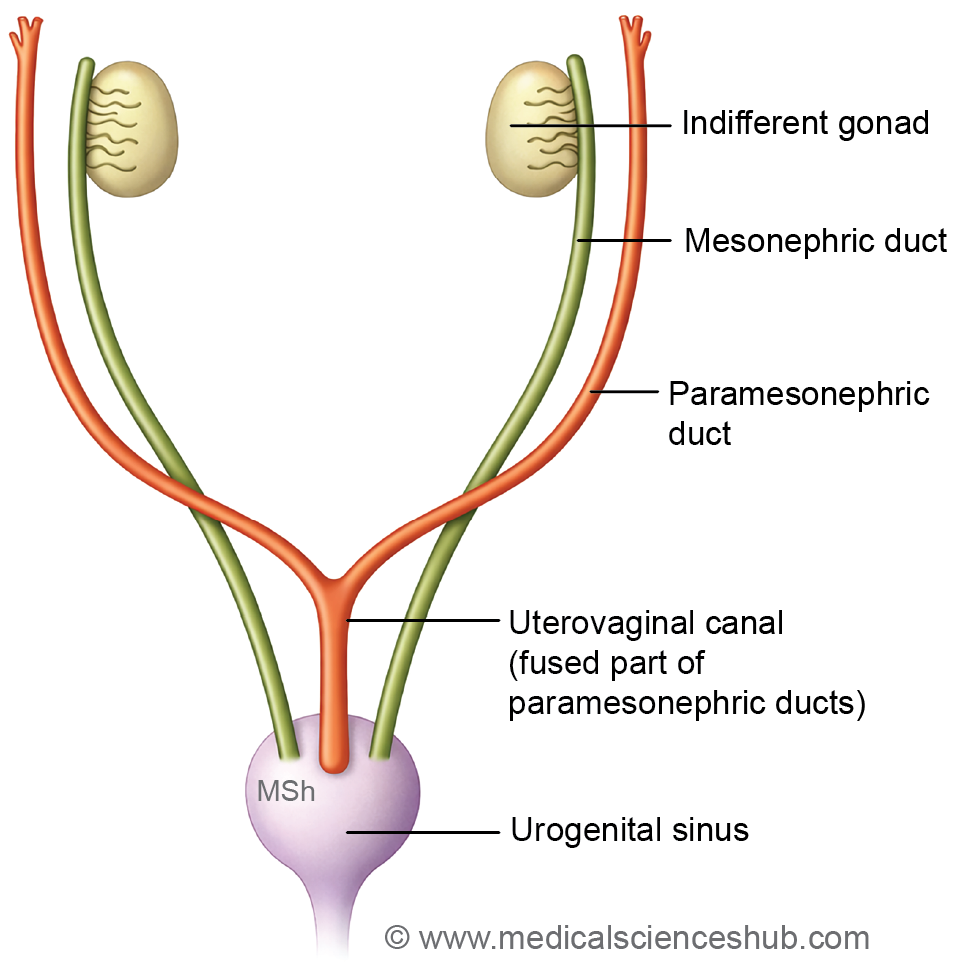
GENITAL DUCTS
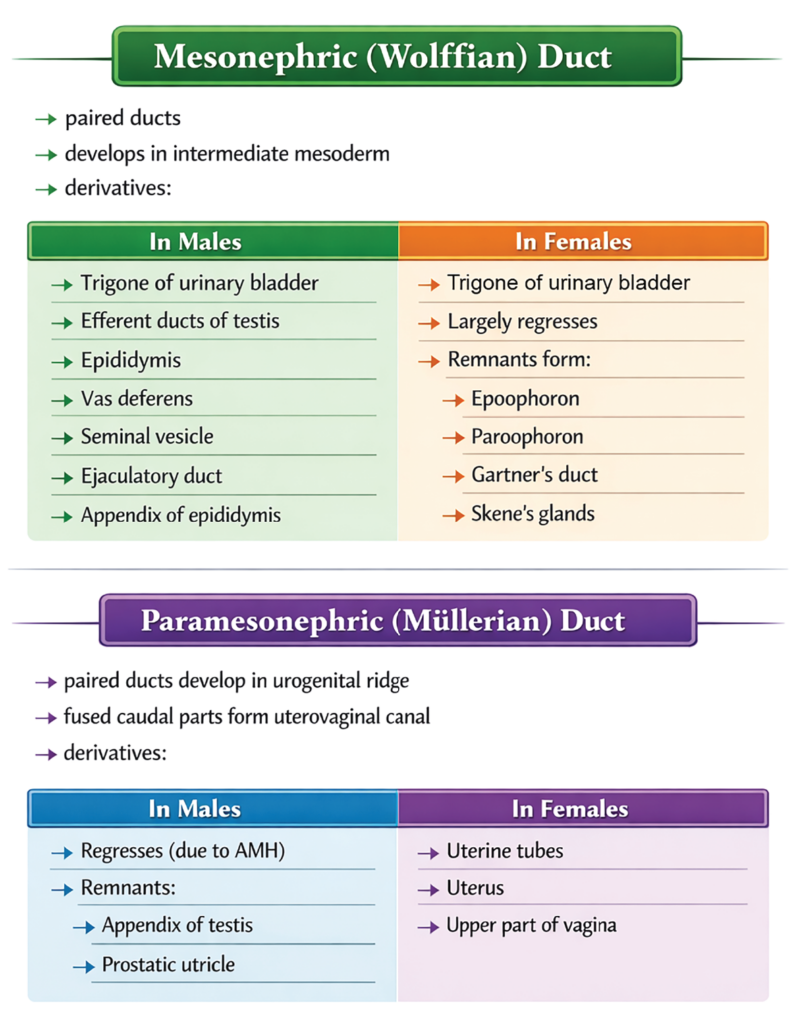
- During early embryonic development, two pairs of primitive ducts contribute to the formation of the reproductive tract: the mesonephric (Wolffian) ducts and the paramesonephric (Müllerian) ducts. These ducts initially coexist in both sexes but later differentiate in a sex-specific manner. The mesonephric ducts predominantly develop into components of the male genital duct system, whereas the paramesonephric ducts give rise to the female reproductive ducts.
Mesonephric Duct (Wolffian Duct)
- The mesonephric duct is a paired tubular structure that develops from the intermediate mesoderm and extends caudally to open into the primitive urogenital sinus. It is also known as the Wolffian duct, archinephric duct, nephric duct, or Leydig’s duct. The mesonephric system was first described by Caspar Friedrich Wolff in 1759.
- In females, the mesonephric ducts largely regress because Anti-Müllerian hormone (AMH) is absent and the ducts are not maintained by testosterone. In contrast, in males these ducts persist and differentiate into several important reproductive structures.
Derivatives of the Mesonephric Duct
In males
- Trigone of the urinary bladder (derived from incorporation of the mesonephric ducts; present in both sexes)
- Efferent ductules of the testis
- Epididymis
- Vas deferens
- Seminal vesicles
- Ejaculatory ducts
- Part of the posterior wall of the prostatic urethra
- Appendix of epididymis
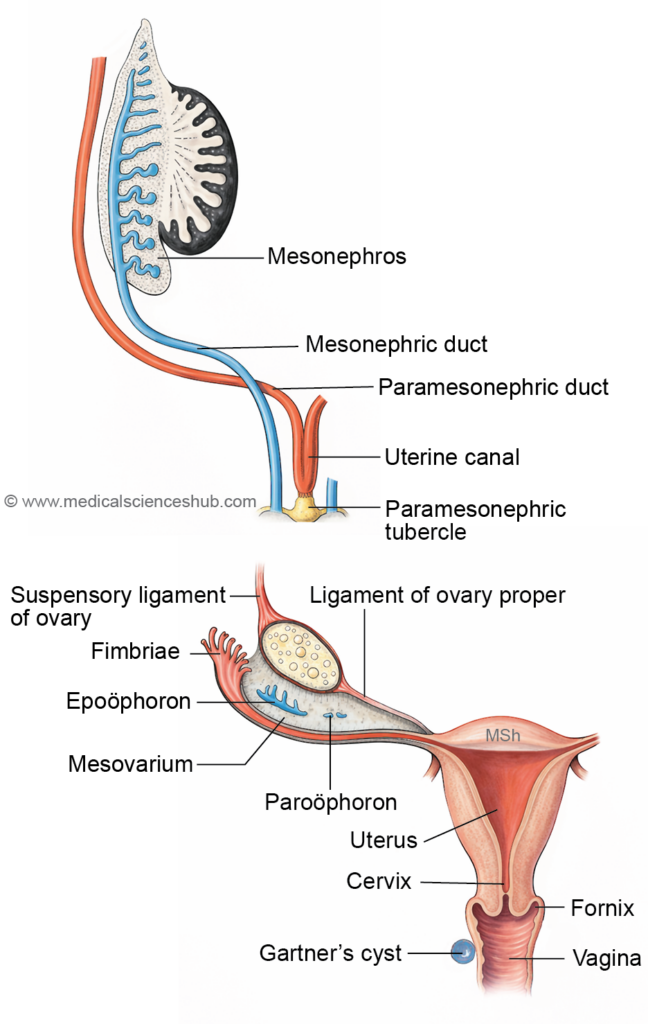
In females (vestigial remnants)
- Trigone of the urinary bladder
- Epoöphoron
- Paroöphoron
- Gartner’s duct or Gartner’s cyst
- Paraurethral glands (Skene’s glands)
The appendix testis (hydatid of Morgagni) represents a remnant of the paramesonephric duct in males and may appear as a small pedunculated structure near the testis.
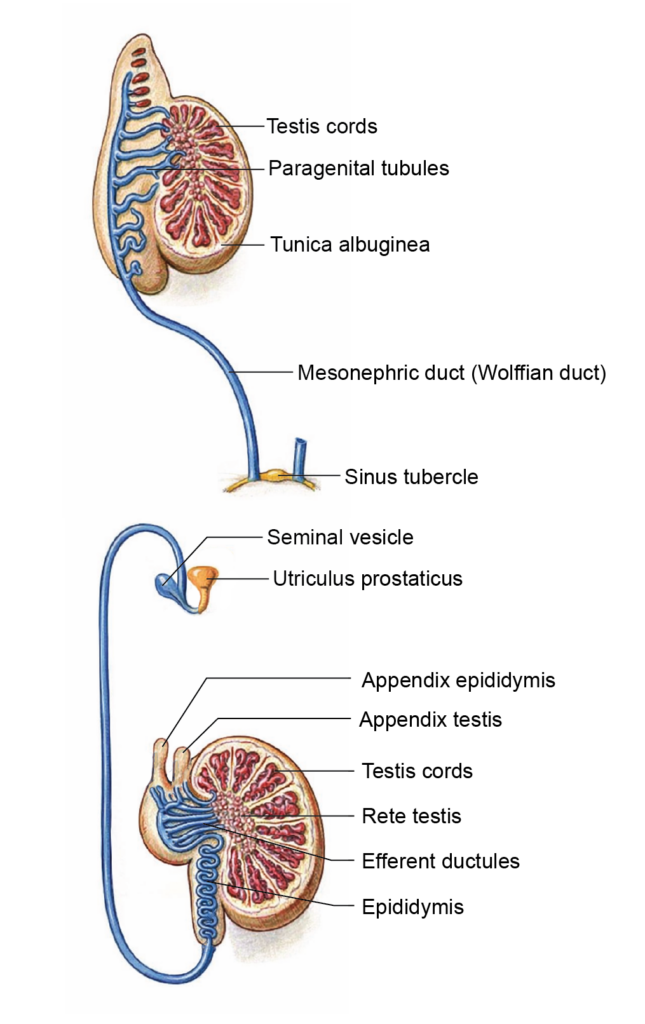
Mesonephric Tubules
Mesonephric Tubules in Male
- In males, several mesonephric tubules persist and differentiate into components of the male reproductive tract. A group of these tubules establishes connections with the developing testis and forms the efferent ductules, which transport sperm from the rete testis to the epididymis.
- Some remaining tubules do not integrate into the main duct system and persist as small vestigial structures, including:
- Superior aberrant ductules
- Inferior aberrant ductules
- Paradidymis (organ of Giraldés)
- These remnants represent residual parts of the embryonic mesonephric system.
Mesonephric Tubules and Duct in Females
- In females, most mesonephric tubules regress but may persist as small vestigial structures. The mesonephric tubules give rise to the epoöphoron and paroöphoron, which are remnants located within the broad ligament of the uterus.
- The mesonephric duct may persist as Gartner’s duct, which sometimes connects with the tubules of the epoöphoron. Together, these structures form the organ of Rosenmüller (epoöphoron), derived from both the mesonephric duct and mesonephric tubules.
- All these remnants—epoöphoron, paroöphoron, and Gartner’s duct—are typically situated in the broad ligament, a peritoneal fold that supports the uterus.
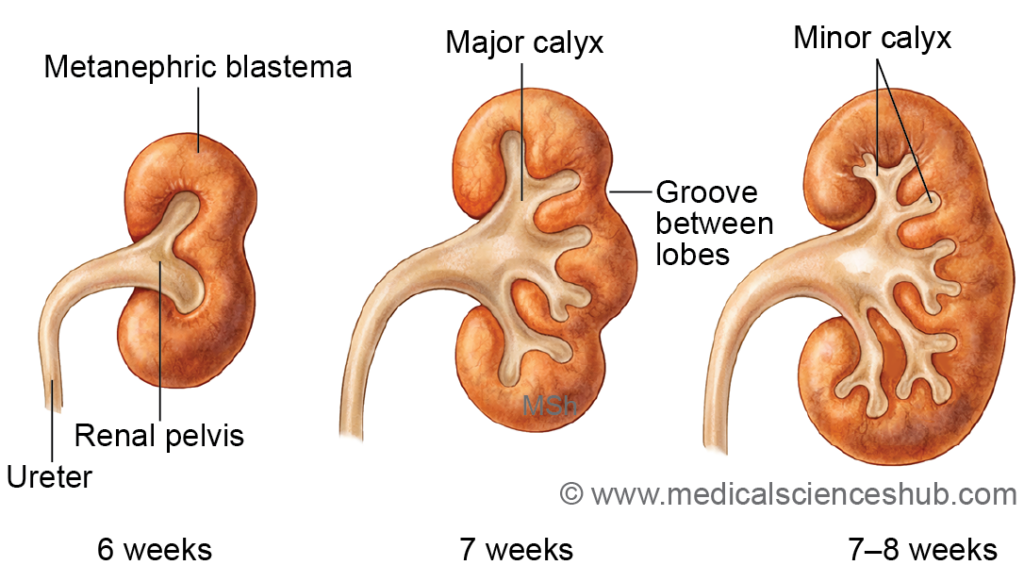
- The ureteric bud arises from the mesonephric (Wolffian) duct. It develops into the ureter, renal pelvis, major and minor calyces, and the collecting tubules of the definitive kidney.
Paramesonephric Duct (Müllerian Ducts)
- The paramesonephric ducts are paired embryonic ducts that develop within the urogenital ridge of the intermediate mesoderm, positioned lateral to the mesonephric ducts.
- Around the 6th week of intrauterine life, the coelomic epithelium lining the peritoneal cavity invaginates into the intermediate mesoderm to form these ducts. As development proceeds, the ducts grow caudally and gradually shift medially. By approximately the third month, they cross ventral to the mesonephric ducts and fuse with each other in the midline, forming the uterovaginal canal. This fused canal later establishes communication with the definitive urogenital sinus.
- The cranial ends of the paramesonephric ducts remain open to the peritoneal (coelomic) cavity, while the caudal fused portion projects into the posterior wall of the urogenital sinus, producing a prominence known as the Müllerian tubercle. During the 8th week, the growing caudal segments pass ventral to the mesonephric ducts and extend toward the region of the urorectal septum.
- In females, the paramesonephric ducts persist because anti-Müllerian hormone (AMH) is absent. In males, however, AMH secreted by Sertoli cells of the developing testis causes regression of these ducts.
Derivatives of the Paramesonephric Duct
In females
- Uterine tubes (fallopian tubes)
- Uterus
- Upper portion of the vagina
In males (vestigial remnants)
- Appendix of testis
- Prostatic utricle (vagina masculina or vesicula prostatica)
The prostatic utricle in males is homologous to the uterus and upper vagina in females.
DEVELOPMENT OF KIDNEYS
- The human kidney develops from two main structural components that form the definitive organ.
- Collecting part: This component includes the collecting tubules, collecting ducts, minor and major calyces, renal pelvis, and ureter.
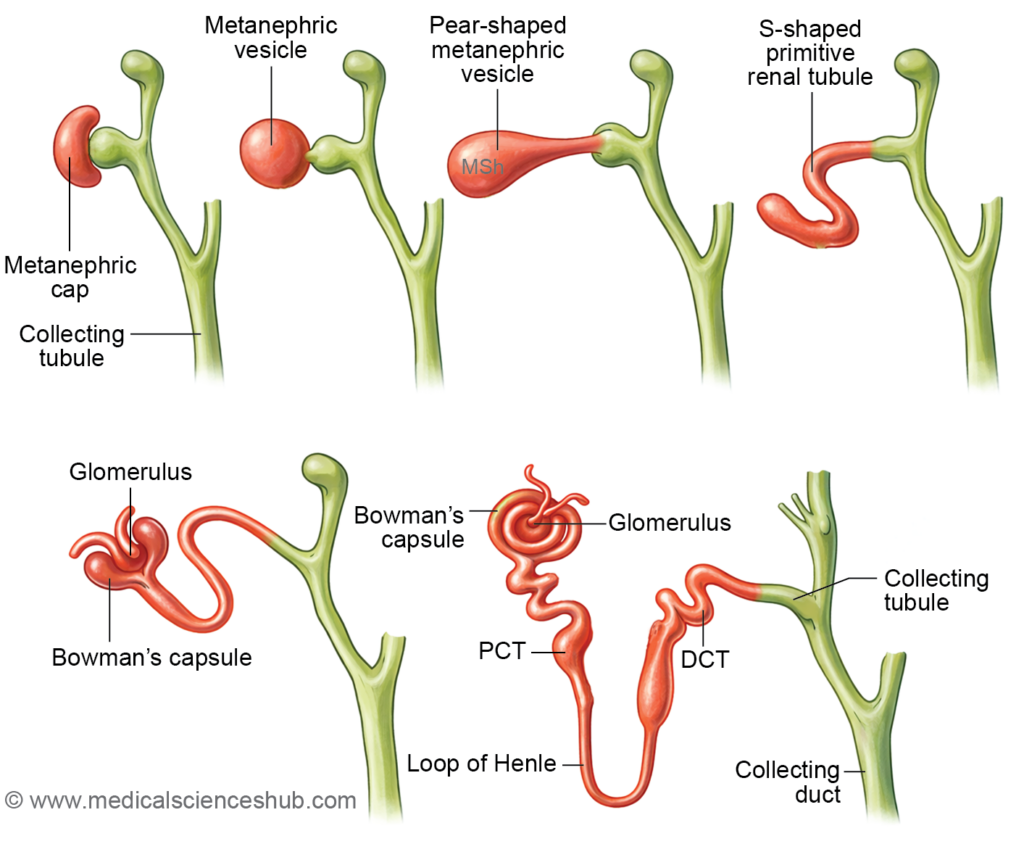
- Secretory part: This portion forms the functional units of the kidney and includes the glomeruli, Bowman’s capsule, proximal convoluted tubules, loop of Henle, and distal convoluted tubules.
Embryological Origin
The two components arise from distinct embryonic sources:
- The ureteric bud gives rise to the collecting system of the kidney.
- The metanephric blastema (metanephric mesenchyme) forms the secretory part, including the nephrons.
Functional Activity
- The fetal kidneys begin to function around the 12th week of intrauterine life, producing urine that is released into the amniotic cavity. Although this urine contributes to the amniotic fluid, fetal waste products are primarily eliminated through the placenta.
Evolutionary History of Kidney
- The kidney develops from the nephrogenic cord, a longitudinal structure derived from the intermediate mesoderm that extends from the cervical to the sacral region of the embryo.
- Kidney development reflects the principle that embryonic stages resemble evolutionary forms. During vertebrate evolution, three major kidney types appear sequentially: pronephros, mesonephros, and metanephros. Primitive vertebrates such as cyclostomes and some teleost fishes possess a pronephric kidney, whereas mesonephric kidneys occur in many fishes and amphibians. In higher vertebrates, including primates and humans, the permanent kidney is the metanephros.
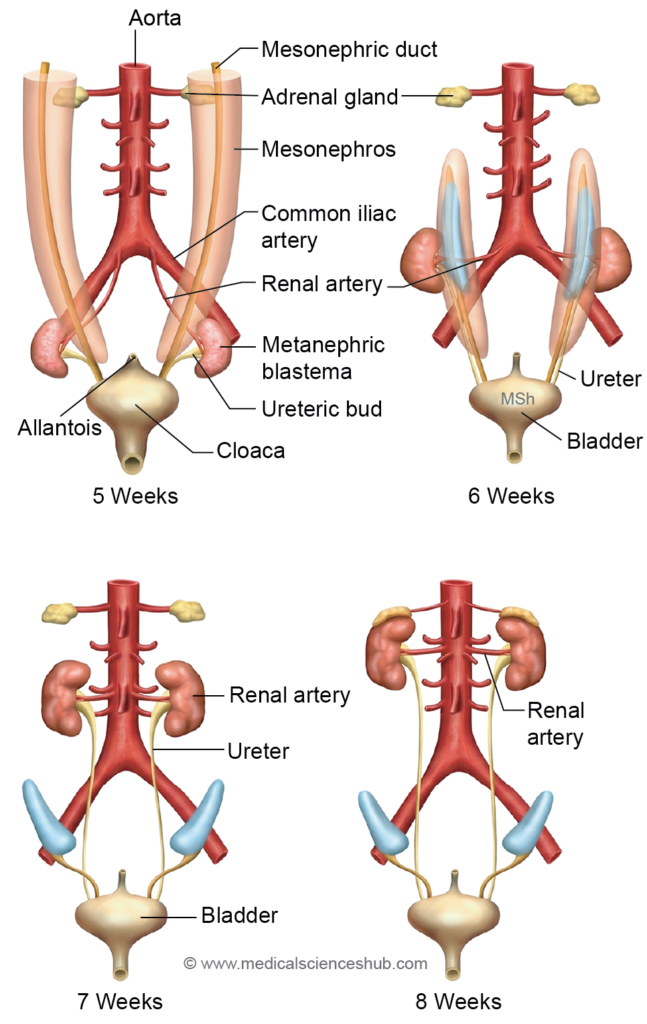
- During human embryonic development, the nephrogenic cord produces three successive renal systems:
- Pronephros – This rudimentary kidney appears in the cervical region at the beginning of the 4th week. It is nonfunctional in humans and rapidly regresses. Its duct persists and becomes the mesonephric duct.
- Mesonephros – This temporary kidney develops in the thoracolumbar region near the end of the 4th week. Most mesonephric tubules degenerate, although some persist in males as the efferent ductules of the testis. The mesonephric duct contributes to parts of the male reproductive tract.
- Metanephros – The permanent kidney begins to develop in the lumbosacral region at the start of the 5th week. It forms the definitive secretory units (nephrons) of the human kidney.
Stages of Kidney Development
- Kidney development occurs through coordinated interactions between the ureteric bud and the metanephric blastema, which together form the collecting and secretory components of the definitive kidney.
- Development of collecting system
- The ureteric bud arises from the caudal part of the mesonephric duct and grows toward the developing metanephros within the nephrogenic cord. The expanding tip of the bud becomes dilated to form an ampulla, which is covered by the metanephric blastema.
- The ampulla undergoes repeated dichotomous branching, usually for about 12–14 generations. These successive divisions produce the structures of the renal collecting system, including the renal pelvis, major calyces, minor calyces, collecting ducts, and collecting tubules.
- Development of secretory (excretory) part
- Cells of the metanephric blastema surrounding the branching ureteric bud differentiate to form the metanephric cap. This tissue condenses and transforms into a metanephric vesicle, which later elongates into an S-shaped primitive renal tubule.
- One end of this tubule enlarges to form Bowman’s capsule, while the opposite end establishes a connection with the collecting tubules derived from the ureteric bud. The primitive tubule subsequently differentiates into the main components of the nephron, including the proximal convoluted tubule, loop of Henle, and distal convoluted tubule.
- A tuft of capillaries derived from nearby mesoderm invaginates Bowman’s capsule, forming the renal corpuscle. Thus, the metanephros ultimately produces the functional secretory unit of the kidney, the nephron, which extends from the renal vesicle to the distal tubule that joins the collecting system.
- Ascent of kidney
- The metanephric kidney initially develops in the pelvic region at the sacral level within the metanephros of the nephrogenic cord. During development, the kidneys gradually migrate upward to reach the thoracolumbar region, attaining their typical abdominal position by approximately the 9th week of intrauterine life.
- Factors responsible for kidney ascent include:
- The need to obtain a more stable arterial blood supply
- Limited space in the pelvic cavity as the kidneys enlarge
- Differential growth of the posterior abdominal wall
- Progressive straightening of the fetal body curvature
- Timeline
- The metanephros appears around the 5th week of intrauterine life.
- By the 9th week, the kidneys usually reach their definitive abdominal position.
- Blood supply of kidney
- During early development, the primitive kidney receives blood from branches of the median sacral artery, a continuation of the abdominal aorta. As the kidneys ascend, they are supplied successively by temporary lateral splanchnic branches of the aorta. Eventually, one of these vessels—usually arising near the L2 vertebral level—persists as the definitive renal artery.
- Rotation of kidney
- When the kidneys reach the thoracolumbar region, each kidney undergoes a medial rotation around its vertical axis. As a result, the renal hilum, which initially faces anteriorly (ventrally), shifts to a medial orientation, the normal position seen in the adult kidney.
CLINICAL EMBRYOLOGY
Congenital Anomalies of Kidney
1. Renal Agenesis
Definition: Complete absence of kidney formation due to failure of the ureteric bud to develop or to induce the metanephric mesenchyme.
Characteristic features:
- Unilateral: usually asymptomatic
- Bilateral: Potter sequence, pulmonary hypoplasia, fatal
Genetic Basis of Renal Agenesis:
The metanephric mesenchyme secretes glial cell line–derived neurotrophic factor (GDNF), which is essential for the induction, branching, and growth of the ureteric bud. Proper interaction between the ureteric bud and metanephric tissue is critical for normal kidney development.
Mutations in genes that regulate GDNF signaling or metanephric differentiation can disrupt this process, leading to renal agenesis. Important genes involved include:
- SALL1 – associated with Townes–Brocks syndrome
- PAX2 – associated with renal coloboma syndrome
- EYA1 – associated with branchio-oto-renal syndrome
These genetic defects impair ureteric bud formation or branching, resulting in failure of kidney development.
2. Duplication (Duplex Collecting System)
Definition: Presence of two ureters or renal pelves caused by early splitting or duplication of the ureteric bud.
Characteristic features:
- Vesicoureteral reflux
- Recurrent urinary tract infections
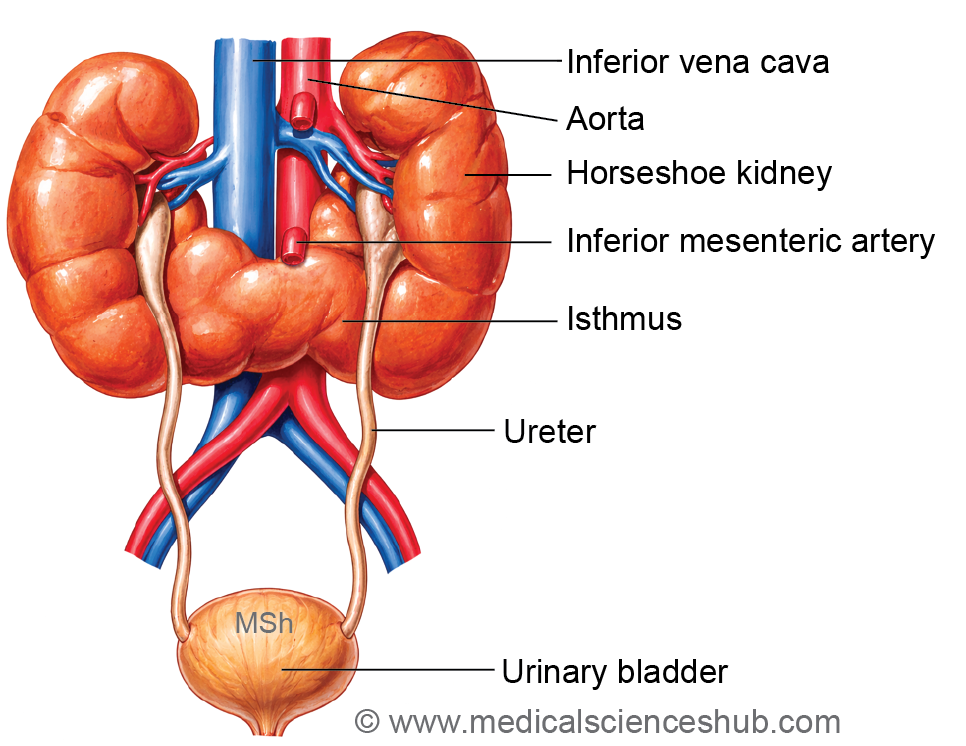
3. Horseshoe Kidney
Definition: Fusion of the lower poles of both kidneys forming a midline isthmus before ascent.
Characteristic features:
- Arrested ascent below inferior mesenteric artery
- Hydronephrosis, renal stones
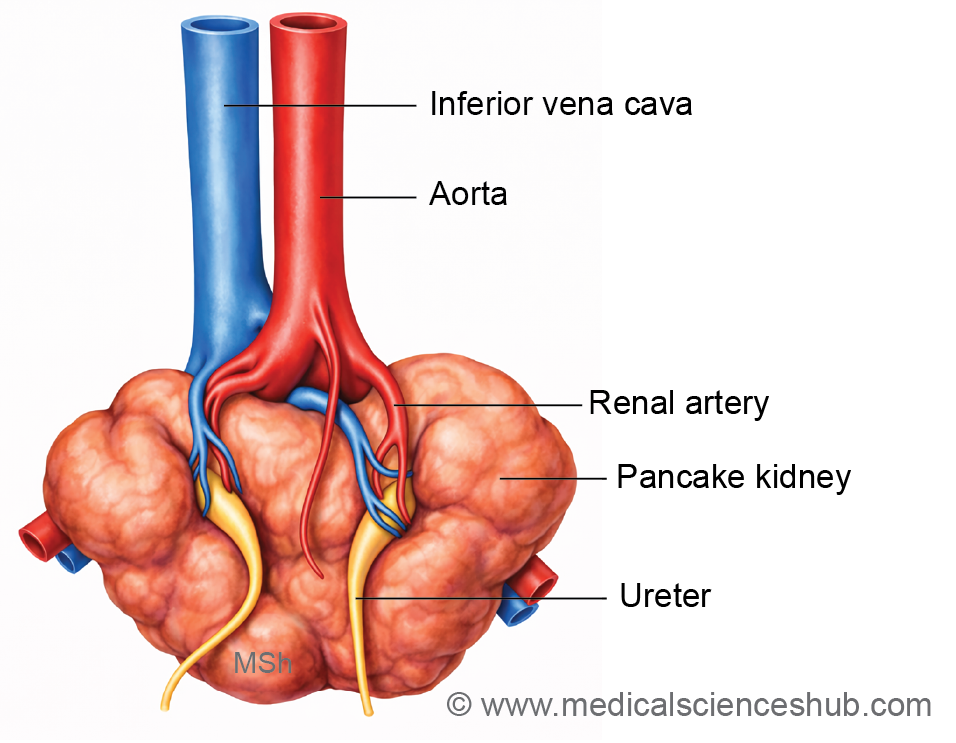
4. Pancake Kidney (Fused Pelvic Kidney)
Definition: Complete fusion of both kidneys into a single mass located in the pelvis due to failure of ascent.
Characteristic features:
- Short ureters
- Often asymptomatic or urinary obstruction
5. Lobulated Kidney
Definition: Kidney is lobulated during development and it disappears in first year of life. Persistence of fetal lobulation due to incomplete fusion of renal lobules forms lobulated kidney.
Characteristic features:
- Normal renal function
- Incidental radiological finding
6. Anomalies of Ascent of Kidney
Definition: Abnormal position of the kidney resulting from defective cranial migration during development.
Abnormal Positions of the Kidney (Anomalies of Ascent)
- Pelvic kidney: The kidney remains in the pelvic cavity due to failure of normal ascent during development.
- Lower lumbar kidney: The kidney ascends partially and is located at the level of the lower lumbar vertebrae.
- Thoracic kidney: The kidney shows excessive ascent, reaching the thoracic cavity, often passing through a diaphragmatic defect.
Characteristic features: Increased risk of obstruction and infection
7. Congenital Polycystic Kidney Disease
Definition: Congenital Polycystic Kidney Disease
Congenital polycystic kidney is characterized by multiple fluid-filled cysts, usually affecting both kidneys (bilateral). It results from defective interaction between the nephron (secretory/excretory segments) and the collecting system, or more precisely, from abnormal dilatation of uriniferous tubules.
Clinical forms:
- Autosomal recessive polycystic kidney disease (ARPKD): A rare form presenting in infancy or early childhood, often with early symptoms.
- Autosomal dominant polycystic kidney disease (ADPKD): A more common form, typically manifesting in adulthood (30–40 years).
Incidence:
- ARPKD: ~1 in 5,000 births
- ADPKD: ~1 in 500–1,000 births
Genetic basis (ADPKD): Commonly due to mutations in PKD1 (chromosome 16) or PKD2 (chromosome 4).
Characteristic features:
- Enlarged kidneys
- Hypertension and progressive renal failure
Management: Advanced disease may require dialysis or kidney transplantation.
8. Accessory Renal Artery
Definition: Persistence of one or more embryonic lateral splanchnic arteries supplying the kidney.
Characteristic features:
- May compress ureter
- Can cause hydronephrosis
9. Wilms’ Tumor (Nephroblastoma)
Definition: Wilms’ tumor is the most common primary renal malignancy in children. It arises from abnormal proliferation of nephrogenic tissue and is strongly associated with mutations in the WT1 gene, located on chromosome 11p13.It’s incidence is common in children age 3-4,after which it is uncommon.
Characteristic features:
- Abdominal mass in children
- Hematuria, hypertension
10. Multicystic Dysplastic Kidney
Definition: Nonfunctional kidney composed of multiple non-communicating cysts due to abnormal interaction between ureteric bud and metanephric tissue.
Characteristic features:
- Unilateral abdominal mass in infants
DEVELOPMENT OF URETER
The ureter develops from the ureteric bud, an outgrowth of the mesonephric (Wolffian) duct. As the ureteric bud elongates and differentiates, the segment between the renal pelvis and the developing urinary bladder (derived from the cloaca) forms the ureter.
CLINICAL EMBRYOLOGY
Anomalies of Ureter
1. Ureteral Agenesis
Definition: Complete absence of the ureter due to failure of the ureteric bud to arise from the mesonephric duct.
Characteristic features:
- Usually associated with renal agenesis
- Absence of urine drainage from affected side
2. Ectopic Ureter
Definition: Abnormal termination of the ureter at a site other than the urinary bladder due to defective incorporation into the bladder wall.
- In males: Contributes to the formation of the lower pa of the urinary bladder, prostatic urethra, seminal vesicles, and rectum.
- In females: Forms the urethra, vagina, vestibule, and rectum.
Characteristic features:Continuous urinary dribbling (especially in females)
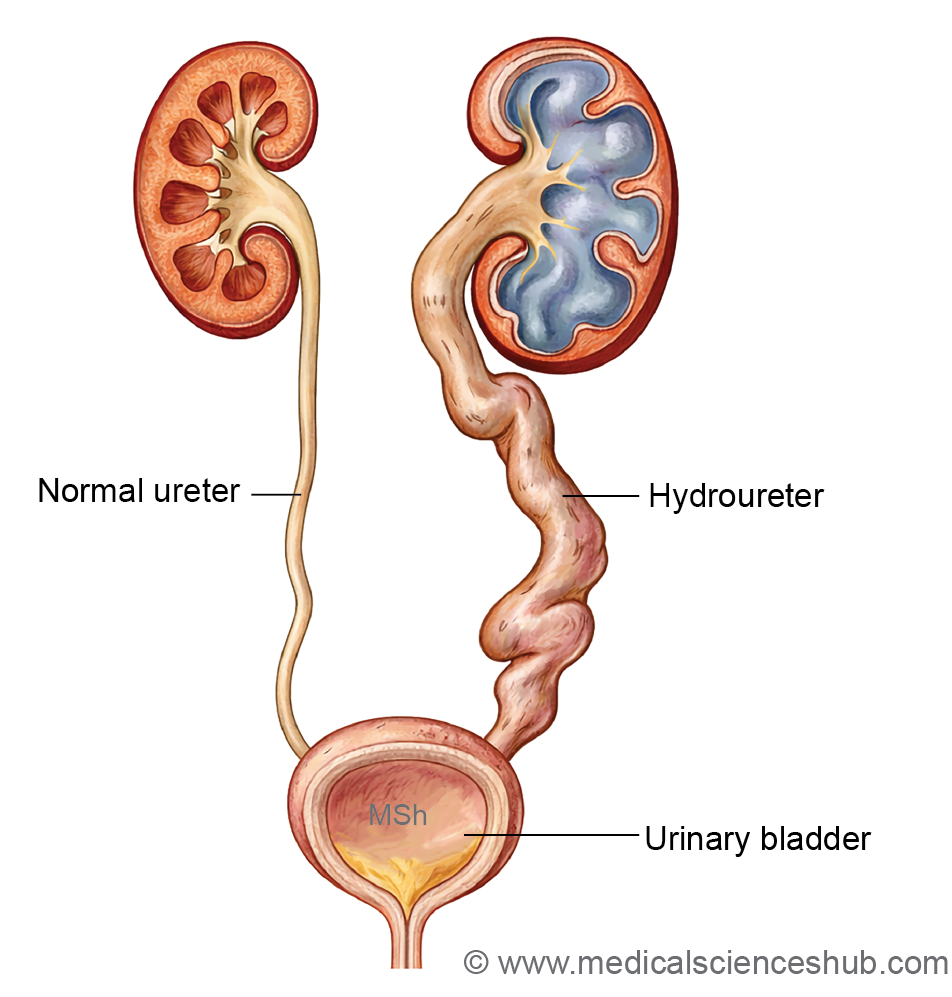
3. Ureteric Obstruction (Hydroureter)
Definition: Dilatation of the ureter due to partial or complete obstruction, often from abnormal lumen formation or external compression.
Characteristic features:
- Dilated ureter (hydroureter)
- May lead to hydronephrosis and renal damage
4. Duplication (Double Ureter)
Definition: Formation of two ureters from a single kidney due to duplication or early division of the ureteric bud.
Characteristic features:
- Two separate openings or partial fusion
- Reflux, obstruction, recurrent infections
5. Blind Ureter
Definition: A ureter that ends blindly without connecting to the kidney, resulting from abnormal branching of the ureteric bud.
Characteristic features:
- No functional drainage
- May form cystic dilatation
6. Bifid Ureter
Definition: Partial duplication in which two ureters unite before entering the bladder.
Characteristic features:
- Usually asymptomatic
- May predispose to urinary infection
7. Ureterocele
Definition: Cystic dilatation of the terminal intramural part of the ureter due to incomplete canalization.
Characteristic features:
- Balloon-like swelling in bladder
- Obstruction and hydronephrosis
8. Retrocaval (Preureteric) Ureter
Definition: Ureter passes posterior to the inferior vena cava due to abnormal development of venous system.
Characteristic features:
- Ureteral compression
- Hydronephrosis and flank pain
9. Congenital Megaur
Definition: Marked dilatation of the ureter caused by defective muscular development or distal obstruction.
Characteristic features:
- Dilated tortuous ureter
- Urinary stasis, infection
DEVELOPMENT OF URINARY BLADDER
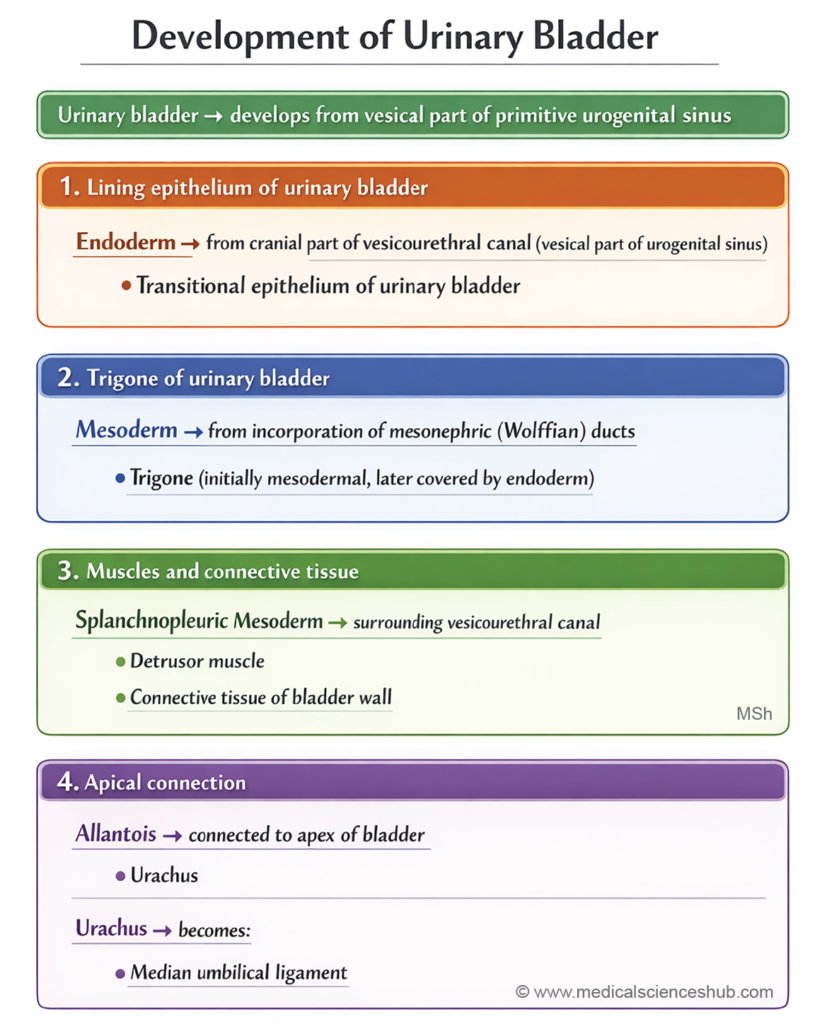
- The urinary bladder consists of an inner transitional epithelium, a middle connective tissue and smooth muscle layer, and an outer serous (connective tissue) layer. Its interior contains a smooth triangular area called the trigone, where the ureters open at the superolateral angles and the internal urethral orifice lies at the apex.
Developmental origin
- The lining epithelium of the bladder (except the trigone) is derived from the cranial dilated part of the vesicourethral canal (endoderm).
- The trigone epithelium originates from mesoderm, formed by incorporation of the mesonephric ducts into the posterior wall.
- The muscle and connective tissue layers develop from splanchnic (visceral) mesoderm surrounding the vesicourethral canal.
- The urachus (future median umbilical ligament) is derived from the allantois.
Stages of Urinary Bladder Development
1. Cloacal Division
- The cloaca is partitioned by the urorectal septum into a ventral urogenital sinus and a dorsal primitive rectum.
- When the septum reaches the cloacal membrane, it divides it into the anterior urogenital membrane and posterior anal membrane, and contributes to formation of the perineal body.
- The cloaca receives the mesonephric ducts and transiently the paramesonephric ducts.
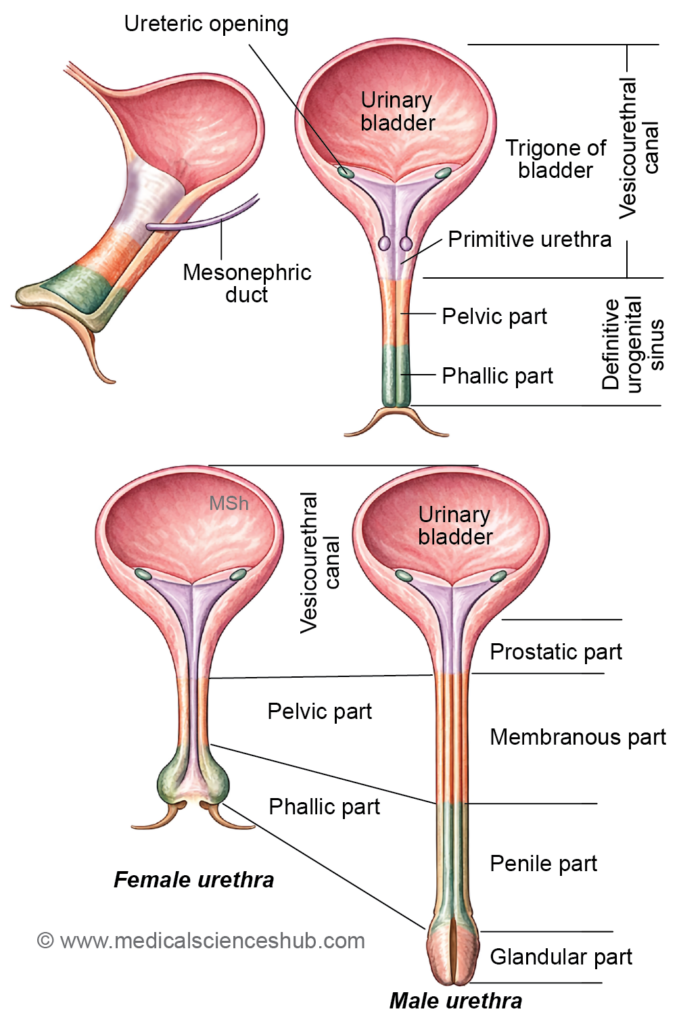
- By the 5th week, the mesonephric ducts open into the urogenital sinus, dividing it into a cranial vesicourethral canal and a caudal definitive urogenital sinus.
- The latter further differentiates into pelvic and phallic parts.
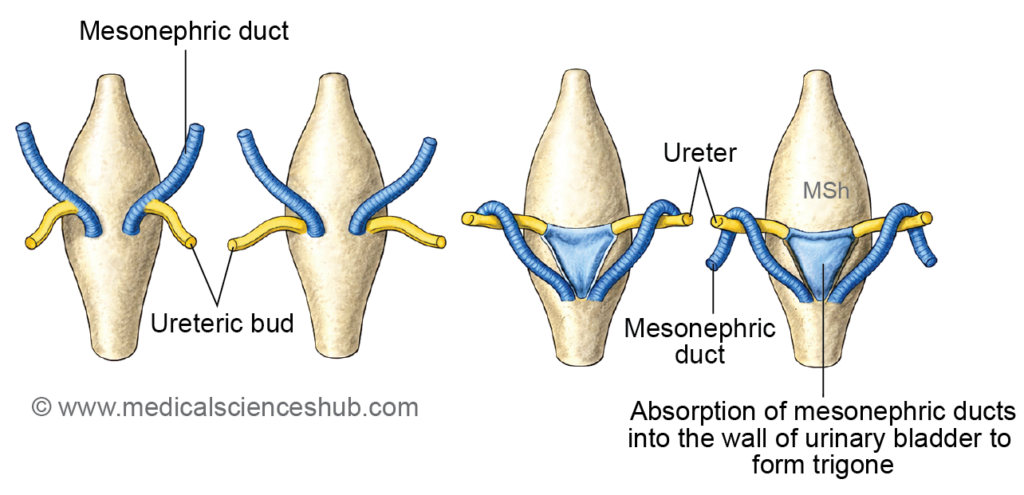
2. Absorption of mesonephric ducts into vesicourethral canal:
- Absorption of Mesonephric Ducts into the Vesicourethral Canal
- Initially, the ureteric buds (future ureters) and mesonephric ducts share a common opening into the vesicourethral canal.
- With progressive incorporation of the mesonephric ducts into its posterior wall, their openings become separated from those of the ureteric buds.
- As development proceeds, the ureteric orifices shift cranially and laterally.
- The incorporated segments of the mesonephric ducts form a triangular area on the posterior wall, known as the trigone of the urinary bladder, located between the openings of the ureters and mesonephric ducts.
- In females, the terminal portions of the mesonephric ducts regress, whereas in males they persist and differentiate into the ejaculatory ducts.
3. Development of muscular and connective tissue coats:
- The muscle and connective tissue layers of the urinary bladder develop from the surrounding splanchnic (visceral) intraembryonic mesoderm that envelops the vesicourethral canal.
CLINICAL EMBRYOLOGY
1. Fistulas:
- Rectovesical fistula: Results from incomplete formation of the urorectal septum, leading to an abnormal connection between the rectum and bladder.
- Vesicovaginal fistula: Occurs due to abnormal positioning of the Müllerian eminence (formed by fused paramesonephric ducts), which may project into the vesicourethral region and create a communication between bladder and vagina.
- Urachal fistula: Caused by persistence of the allantois, resulting in a patent tract between the urinary bladder and the umbilicus.
2. Urachal cyst: Develops from partial persistence of the allantois, specifically its middle segment, forming a midline cystic swelling in the anterior abdominal wall.
3. Urachal sinus: Arises from persistence of the distal part of the allantois, presenting as an opening at the umbilicus.
4. Hourglass bladder: A rare anomaly in which the urinary bladder is divided into upper and lower compartments by a midline constriction.
5. Epispadias: Urethral opening located on the dorsal surface of the penis (male) or anterior to normal position (female) due to defective genital tubercle development.
Characteristic features:
- Urinary incontinence
- Frequently associated with bladder exstrophy
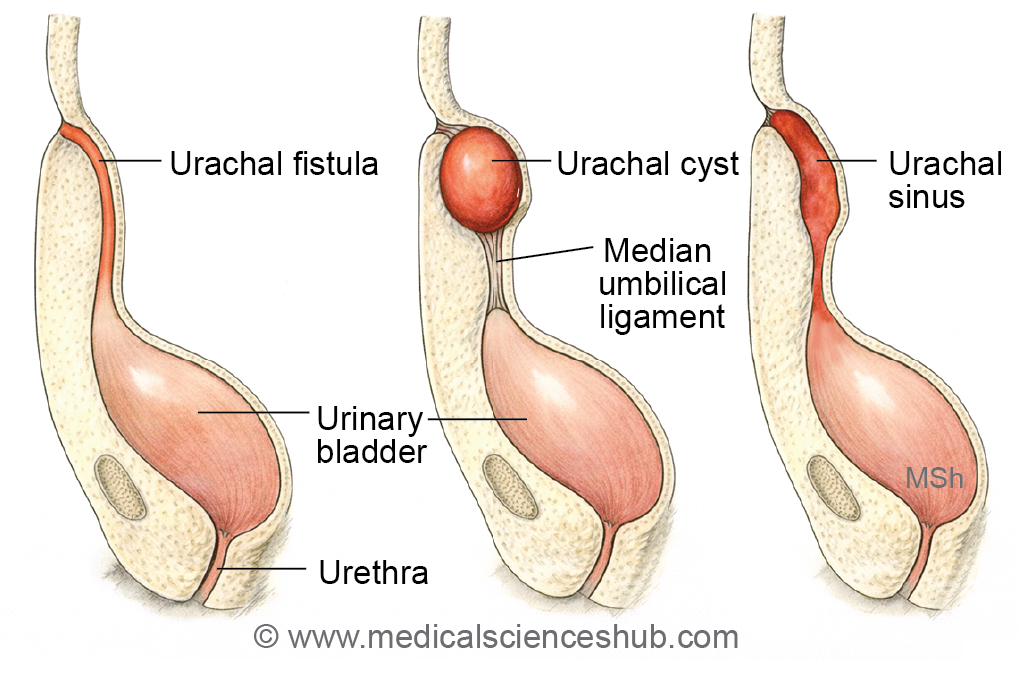
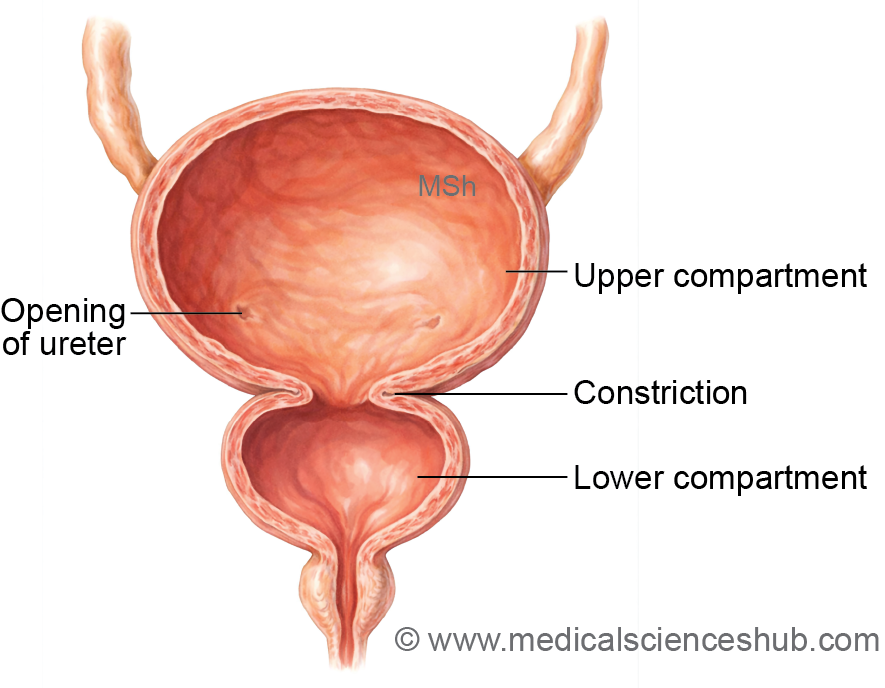
Table 19.1: Development of urinary bladder
| Component | Origin |
|---|---|
| Epithelium (except trigone) | Endoderm of cranial vesicourethral canal |
| Trigone epithelium | Mesoderm from incorporated mesonephric ducts |
| Muscle & stroma | Splanchnopleuric mesoderm |
| Apex (urachus) | Allantois → median umbilical ligament |
DEVELOPMENT OF URETHRA
Development of Female Urethra
- The female urethra is a short tubular structure measuring approximately 4 cm. It develops primarily from the caudal part of the vesicourethral canal.
- The terminal segment is derived from the pelvic part of the definitive urogenital sinus (endodermal origin). A small portion of the dorsal wall arises from incorporated mesonephric ducts (mesodermal contribution) within the vesicourethral canal.
- Developmentally, the female urethra corresponds to the prostatic urethra in males.
Development of Male Urethra
- The male urethra is divided into prostatic, membranous, spongy, and glandular parts. Its development involves contributions from different segments of the vesicourethral canal and urogenital sinus.
- The caudal part of the vesicourethral canal (primitive urethra) forms the upper prostatic urethra, above the openings of the ejaculatory ducts.
- The pelvic part of the definitive urogenital sinus gives rise to the lower prostatic urethra (below the ejaculatory duct openings) and the membranous urethra.
- The phallic part of the urogenital sinus forms most of the spongy urethra, while the terminal glandular segment develops from surface ectoderm.
Table 19.2: Development of urethra
| Segment | Embryological Origin |
|---|---|
| Prostatic (above ejaculatory ducts) | Endoderm of caudal vesicourethral canal (primitive urethra) |
| Prostatic (below ducts) | Pelvic part of urogenital sinus |
| Membranous part | Pelvic urogenital sinus |
| Spongy (penile) part | Phallic urogenital sinus |
| Glandular (terminal glans) | Surface ectoderm |
CLINICAL EMBRYOLOGY
Ectopia Vesicae (Bladder Exstrophy)
- Ectopia vesicae, also known as bladder exstrophy, is a congenital defect characterized by absence of the infraumbilical anterior abdominal wall and the anterior wall of the urinary bladder.
- As a result, the bladder mucosa is exposed, and urine continuously leaks from the open surface.
- It’s incidence is approximately 1 in 10,000 births.
- It is associated with epispadias.
Embryological basis
This anomaly results from failure of proper mesodermal migration and incomplete formation of the lateral body folds, leading to defective closure of the anterior abdominal wall.
Important Questions
- Describe the formation, course, and derivatives of the mesonephric (Wolffian) duct.
- Explain the development and derivatives of the paramesonephric (Müllerian) ducts.
- Outline the embryological development of the kidney, including its stages.
- Describe the ascent of the kidney, including its vascular changes and clinical significance.
- Discuss the congenital anomalies of the kidney, with special reference to horseshoe kidney and unilateral renal agenesis.
- Explain the development of the urinary bladder, including its embryonic origin and differentiation.
- Describe the structure, subdivisions, and derivatives of the primitive urogenital sinus.
- Enumerate and briefly explain the congenital anomalies of the urinary bladder.
- Outline the development of the urethra, including its embryological origin.
- Describe the development of the male urethra, highlighting its different parts and sources.
- Explain the embryological basis, features, and clinical significance of ectopia vesicae (bladder exstrophy).
