Competencies
- AN43.4: Describe the development and developmental basis of congenital anomalies of face, palate (included in this chapter), tongue, branchial apparatus, pituitary gland, thyroid gland, eye.
The human face emerges through a precise sequence of embryonic events in which small facial prominences grow, merge, and remodel. These coordinated transformations shape the nose, lips, and palate, establishing the basic architecture essential for breathing, feeding, speech, and expression.
DEVELOPMENT OF FACE
- The bilateral mandibular processes fuse in the midline to form the lower lip and the mandible.
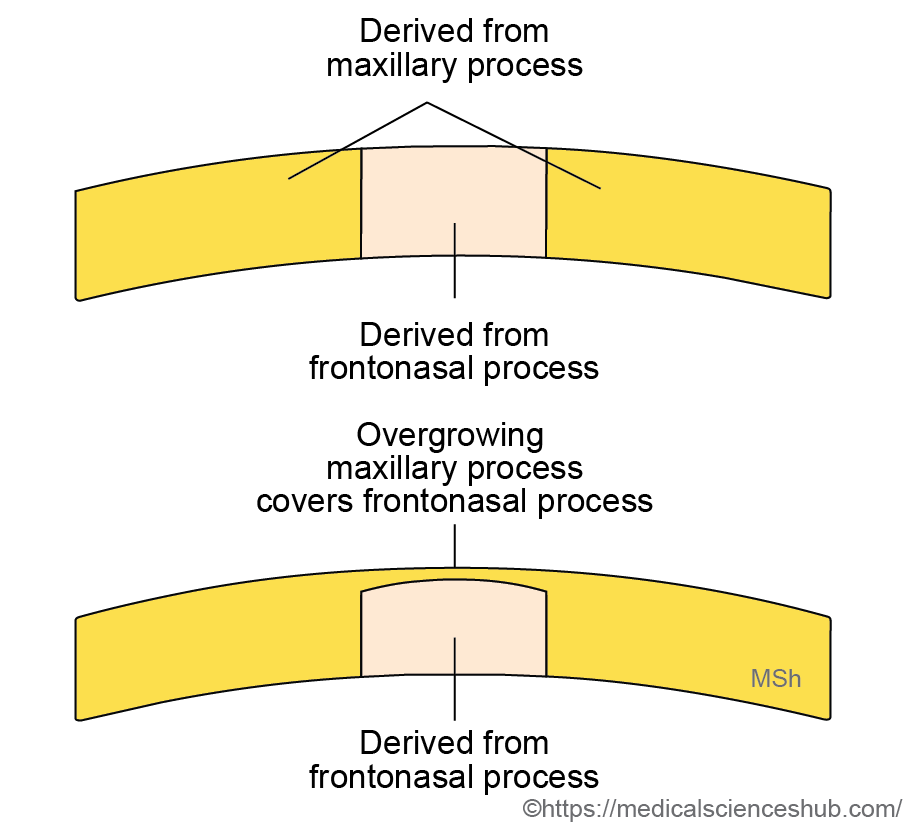
- The central portion (philtrum) of the upper lip develops from the medial nasal processes.
- The lateral portions of the upper lip are formed by the maxillary processes on each side.
- The ectoderm of the maxillary process grows over and covers the philtrum. Consequently, the skin of the upper lip receives sensory supply from the maxillary nerve.
- The muscles of facial expression originate from the second pharyngeal arch and are therefore innervated by the facial nerve.
- The primitive mouth, or stomodeum, is bordered by the maxillary, mandibular, and frontonasal processes.
- Fusion between the maxillary and mandibular processes occurs from the lateral side, reducing the width of the stomodeum to form the normal oral fissure, while the fused lateral region develops into the cheek.
Steps in Development of Face
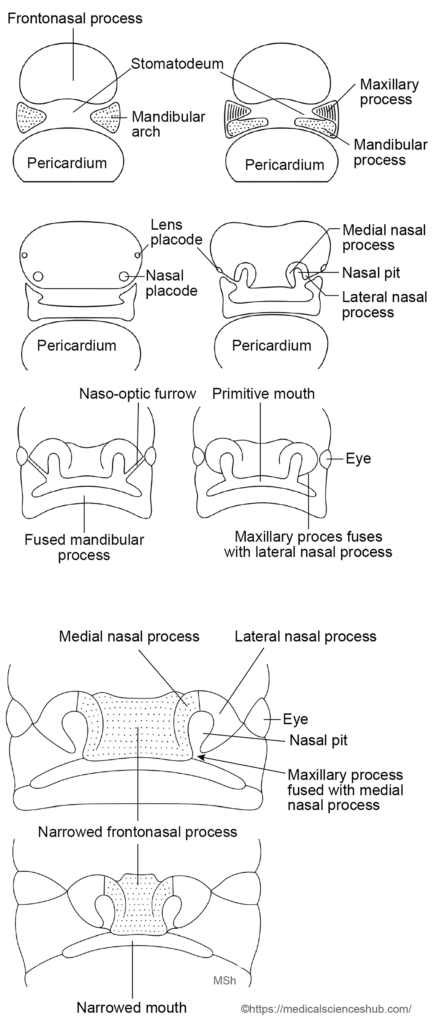
The face develops during the 4th week of embryonic life from five mesenchymal prominences that surround the primitive mouth, known as the stomodeum. These prominences arise from proliferation of underlying mesenchyme beneath the surface ectoderm.
The five facial prominences are:
- Frontonasal prominence (unpaired)
- Maxillary prominences (paired)
- Mandibular prominences (paired)
These structures appear as elevations around the stomodeum and progressively enlarge and fuse to form the facial components.
Most facial development occurs between the 4th and 8th weeks of intrauterine life. By the end of the 8th week, the embryo begins to show a recognizable human facial form. The definitive facial appearance is achieved later through gradual changes in the size, proportions, and relative positions of facial structures during the fetal period.
- During the 4th week of intrauterine life, the stomodeum (primitive mouth) is bounded superiorly by the developing forebrain vesicle and inferiorly by the first pharyngeal (mandibular) arch.
- In the 5th week, mesenchymal proliferation over the forebrain forms the frontonasal prominence. On its surface, paired ectodermal thickenings called nasal (olfactory) placodes appear on either side of the midline.
- Each nasal placode invaginates to form a nasal pit, which later deepens and establishes continuity with the roof of the stomodeum. The margins of each pit rise as horseshoe-shaped ridges that form the medial nasal process (medial border) and lateral nasal process (lateral border).
- While these structures develop, the maxillary processes arise from the cranial part of the first pharyngeal arch. They grow medially and fuse with the medial nasal processes, and subsequently approach the lateral nasal processes.
- Lateral and cranial to the nasal placodes, a pair of lens placodes appears, marking the early site of eye development.
- Between the 7th and 10th weeks, fusion of the maxillary, medial nasal, and lateral nasal processes separates the nasal pits from the stomodeum, forming the primitive anterior nares. Continued growth of these structures produces the bridge of the nose.
- Fusion of the medial nasal processes creates the intermaxillary segment, which forms the philtrum of the upper lip, the premaxillary part of the maxilla, and the primary (primitive) palate.
- The upper lip is mainly derived from the maxillary processes, while its central portion (philtrum) originates from the fused medial nasal processes and is later covered by the medially expanding maxillary tissue.
- The lateral nasal processes do not contribute to the upper lip; they form the alae of the nose.
- The stomodeum becomes separated from the pericardial bulge by the first pharyngeal arch and subsequently by the developing pharyngeal arches.
- The mandibular processes fuse in the midline to form the lower lip, chin, and part of the cheeks.
- Both the maxillary processes and mandibular processes arise from the first pharyngeal arch. Their fusion at the lateral margins contributes to the formation of the angles of the mouth.
- Fusion between the maxillary and mandibular processes continues laterally, which reduces the width of the primitive oral opening (stomodeum) and leads to the formation of the cheeks.
- Nerve supply: Structures derived from the frontonasal prominence receive sensory innervation from the ophthalmic nerve (V1). Derivatives of the maxillary process are supplied by the maxillary nerve (V2), while derivatives of the mandibular process are innervated by the mandibular nerve (V3).
Development of nasolacrimal duct
- The maxillary process grows medially and fuses with the lateral nasal process along the nasolacrimal (naso-optic) groove.
- During this fusion, a strip of ectodermal cells within the groove becomes embedded in the underlying mesenchyme, forming a solid epithelial cord. This cord later undergoes canalization to form the nasolacrimal duct. The superior portion of this duct enlarges to form the lacrimal sac.
- Failure of proper canalization results in atresia or obstruction of the nasolacrimal duct, which may lead to impaired drainage of tears.
Table 12.1: Structures contributing development of the face
| Embryonic Facial Process | Major Structures Derived |
|---|---|
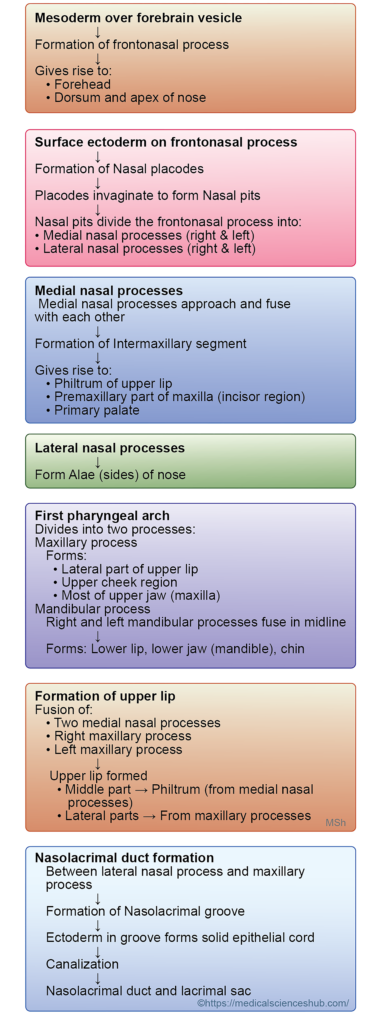
| Frontonasal Process | Forms the forehead, the bridge (dorsum) of the nose, and gives rise to the medial nasal processes and lateral nasal processes, which participate in the formation of nasal and upper facial structures. |
| Medial Nasal Processes | Fuse in the midline to form the philtrum of the upper lip, the crest and tip of the nose, and contribute to the intermaxillary segment, which is important in upper lip development. |
| Lateral Nasal Processes | Develop into the alae (wings) of the nose, forming the lateral boundaries of the nostrils. |
| Maxillary Processes | Give rise to the cheeks and the lateral portions of the upper lip. These processes also fuse with the medial nasal processes during formation of the upper lip. |
| Mandibular Processes | Form the lower lip, lower jaw region, and contribute to the lower facial contour. |
CLINICAL EMBRYOLOGY
- Developmental Anomalies of Face
- Oblique facial cleft occurs when the maxillary process fails to fuse with the lateral nasal process. This defect produces a cleft extending from the medial angle of the eye to the mouth and is often associated with absence or malformation of the nasolacrimal duct.
- Macrostomia refers to an abnormally wide mouth, resulting from incomplete fusion between the maxillary and mandibular processes
- Microstomia is an abnormally small oral opening caused by excessive fusion of the maxillary and mandibular processes
- Proboscis is a rare anomaly characterized by a tubular, elongated nasal structure. It may occur with severe craniofacial defects such as cyclopia, where the two eyes are partially or completely fused.
- Retrognathia describes a small or receding mandible, in which the chin lies posterior to the normal facial profi
- Agnathia is the complete absence of the jaw, usually due to failure of mandibular development.
- Hypertelorism refers to widely spaced eyes, typically associated with a broad nasal bridge resulting from excessive width of the frontonasal prominence
DEVELOPMENT OF NOSE
The external nose and related nasal structures develop from the frontonasal prominence and the associated nasal processes.
- The bridge of the nose is formed from the frontonasal prominence.
- The dorsum and tip of the nose develop from the fused medial nasal processes.
- The alae (wings) of the nose arise from the lateral nasal processes.
- The anterior nares (nostrils) originate from the nasal pits.
- The nasal cavities develop from the nasal sacs, which form as the pits deepen.
- The posterior nares (choanae) are established after rupture of the bucconasal membrane, creating communication between the nasal cavity and the primitive pharynx.
Stages of Development of Nose and Cavities
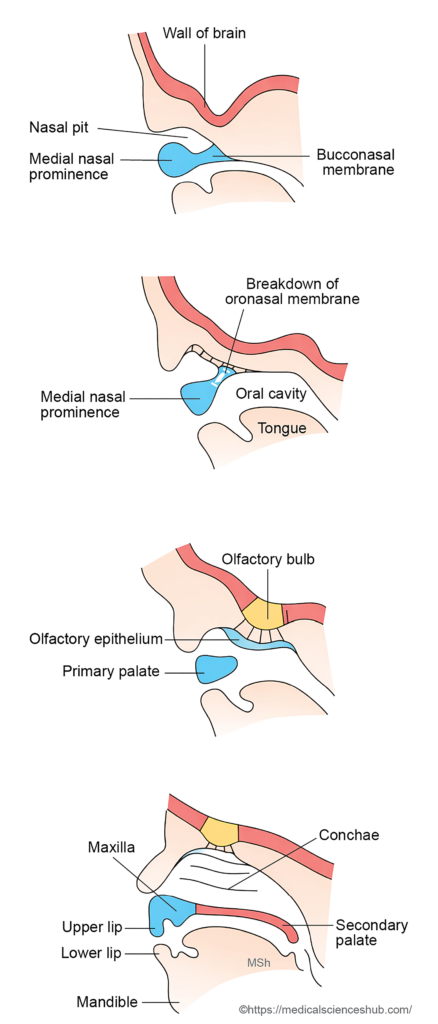
- During early facial development, paired nasal pits appear on the frontonasal prominence. These pits deepen and gradually extend toward the stomodeum, establishing an early connection with the primitive oral cavity.
- The raised margins surrounding each nasal pit form the medial nasal processes and lateral nasal processes. The maxillary processes grow medially and fuse first with the lateral nasal processes and later with the medial nasal processes. Fusion between the medial nasal processes also occurs. As the palate develops, the nasal pits become separated from the stomodeum and form the anterior nares (nostrils).
- As development continues, each nasal pit deepens to form a nasal sac. The sac enlarges dorsally and caudally. Above the primitive palate, it is initially separated from the stomodeum by a thin bucconasal membrane (nasal fin). Subsequent rupture of this membrane establishes communication between the nasal cavity and the oral cavity, producing the posterior nasal apertures (choanae).
- Progressive narrowing of the frontonasal prominence brings the two nasal sacs closer together. This region forms the nasal septum and contributes to the bridge of the nose.
- The medial nasal processes give rise to the dorsum and tip of the nose, whereas the expanding lateral nasal processes form the lateral walls of the nose. Internal elevations within the lateral nasal wall develop into the nasal conchae (turbinates).
- The olfactory epithelium, containing sensory receptor cells, develops from the thickened ectoderm lining the roof of the nasal cavity. The olfactory nerves arise from neural processes extending from the olfactory bulb of the brain to these receptor cells.
Development of paranasal air sinuses
- The paranasal air sinuses develop from ectodermal outgrowths of the nasal cavity.
- Small epithelial diverticula (outpouchings) arise from the nasal cavity and extend into the surrounding bones, including the maxilla, ethmoid, sphenoid, and frontal bones.
- These diverticula gradually enlarge within the bones to form the paranasal sinuses, while their original openings remain as the sinus ostia that communicate with the nasal cavity.
- Most paranasal sinuses begin their development before birth. However, the frontal sinus develops later, usually appearing around the 5th or 6th year of life.
- The maxillary sinus is the first to appear, beginning in the third month of intrauterine life. Growth and expansion of the sinuses continue throughout childhood and typically reach completion around puberty.
DEVELOPMENT OF PALATE
- The palate develops from two embryological components: the primary palate and the secondary palate.
- The primary palate originates from the frontonasal prominence, while the secondary palate develops from the palatine processes of the maxillary prominences. During development, these structures grow toward each other and fuse to form the definitive palate, separating the oral cavity from the nasal cavity.
- In the completed palate, the anterior three-quarters undergo ossification to form the hard palate, whereas the posterior one-quarter remains muscular and forms the soft palate and uvula.
Stages of Palate Development
- Palatogenesis occurs between the 5th and 12th weeks of intrauterine life.
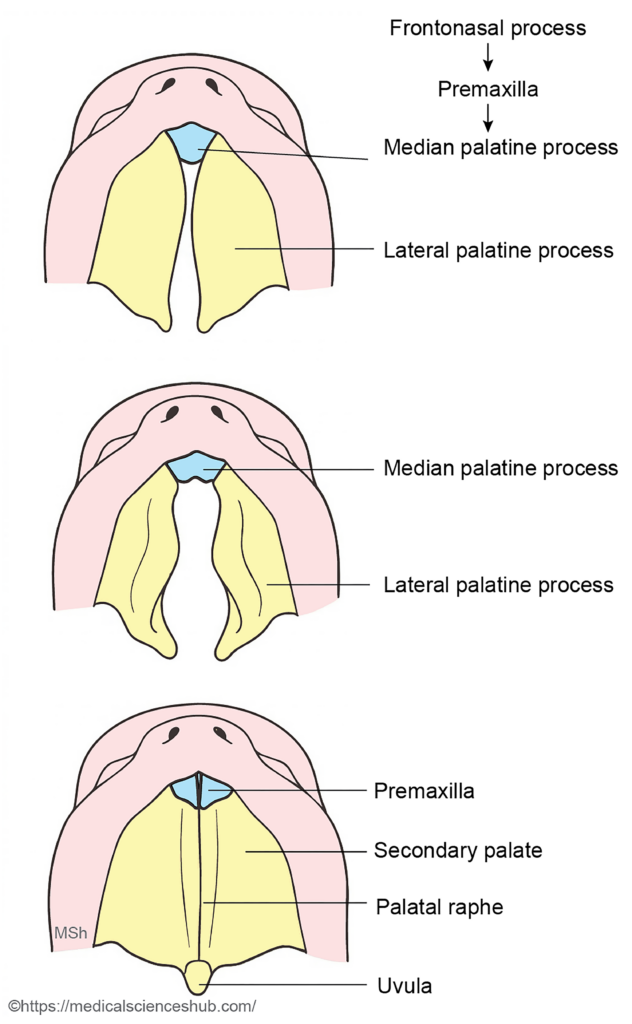
- Primary palate: During the 6th week, the intermaxillary segment forms a shelf-like projection called the primary palate (or median palatine process). This structure later develops into the premaxillary part of the maxilla, which carries the upper four incisor teeth.
- Secondary palate: At approximately the same time, two mesenchymal projections arise from the inner surfaces of the maxillary processes. These are the lateral palatine processes, which form the secondary palate.
- Fusion stage: During the 7th–8th weeks, the lateral palatine processes enlarge and fuse:
- With each other in the midline
- With the nasal septum
- With the posterior margin of the primary palate
- Formation of the definitive palate: Fusion of the primary and secondary palates produces the definitive palate, which separates the oral and nasal cavities. The incisive foramen marks the boundary between the primary and secondary palates.
- The anterior three-quarters undergo ossification to form the hard palate.
- The posterior one-quarter remains muscular and forms the soft palate and uvula.
- A small nasopalatine canal persists in the premaxilla, opening into the incisive fossa through the right and left incisive canals.
- Muscles of the palate: Mesoderm from the pharyngeal arches migrates into the developing soft palate to form its muscles.
- Tensor veli palatini develops from the first pharyngeal arch.
- Levator veli palatini, palatoglossus, palatopharyngeus, and musculus uvulae arise from the fourth pharyngeal arch.
Intermaxillary segment
The intermaxillary segment develops from the fusion of the two medial nasal processes and lies between the maxillary processes during facial development.
This segment differentiates into three components:
- Labial component – forms the philtrum of the upper lip.
- Upper jaw component – gives rise to the premaxillary part of the maxilla, which carries the upper four incisor teeth.
- Palatal component – forms the triangular primary palate, contributing to the anterior part of the definitive palate.
CLINICAL EMBRYOLOGY
Cleft lip (harelip)
- Cleft lip is a congenital defect characterized by a split in the upper lip, occurring on one or both sides of the midline. It may present as unilateral, bilateral, or rarely midline clefts. The term harelip originates from the naturally divided upper lip seen in a hare
- Embryological basis: This anomaly usually results from failure of fusion between the maxillary process and the medial nasal process (a derivative of the frontonasal prominence). A midline cleft lip occurs when the two medial nasal processes fail to fuse.
- Epidemiology:
- Occurs in approximately 1 in 1000 births.
- More common in males than females (about 80% of cases).
- The risk increases slightly with advanced maternal age.
- If a couple has one affected child, the recurrence risk is about 4%; if two children are affected, the risk increases to about 9%.
- Management: The defect can be corrected by surgical reconstruction, usually performed during early infancy.
Cleft Palate
- Cleft palate is a congenital fissure of the palate that creates an abnormal communication between the oral cavity and the nasal cavity. This condition commonly leads to feeding difficulties, speech abnormalities, and dental problems. The most frequent cause is multifactorial inheritance, involving genetic and environmental factors.
- Incidence:
- Occurs in about 1 in 2500 births.
- More common in females (approximately two-thirds of cases).
- Unlike cleft lip, its occurrence is not strongly related to maternal age.
- If one child is affected, the recurrence risk for another child is about 2%.
- Unilateral cleft lip, with or without cleft palate, is the most frequent congenital facial anomaly.
- Embryological basis: Cleft palate results from failure of fusion between the lateral palatine processes, the primary palate (median palatine process), and the nasal septum.
- Classification:
- Complete cleft palate: The cleft extends through both the hard and soft palate and may be unilateral or bilateral.
- Unilateral complete cleft palate occurs when one lateral palatine process fails to fuse with the primary palate and also fails to unite with the opposite palatine process. It is usually associated with cleft lip on the same side.
- Bilateral complete cleft palate results from failure of fusion of both lateral palatine processes with the primary palate.
- Incomplete cleft palate: The defect may involve the hard palate, soft palate, or only the uvula.
- Management: Treatment primarily involves surgical repair, often combined with speech therapy and dental care to restore normal function.
Important Questions
- List the embryonic facial processes that contributes to the development of the face.
- Write a short note the development of palate.
- Write a short note on intermaxillary segment.
- Write a short note on cleft palate and cleft lip.
