Competencies
- AN77.4: Describe the stages and consequences of fertilization.
- AN78.1: Describe cleavage and formation of blastocyst.
- AN78.2: Describe the development of trophoblast
- AN78.3: Describe the process of implantation and common abnormal sites of implantation.
INTRODUCTION
- The first week of human development begins with fertilization, which is the fusion of a secondary oocyte and a spermatozoon, and ends with the initiation of implantation, when the developing conceptus starts to embed within the endometrium of the uterus.
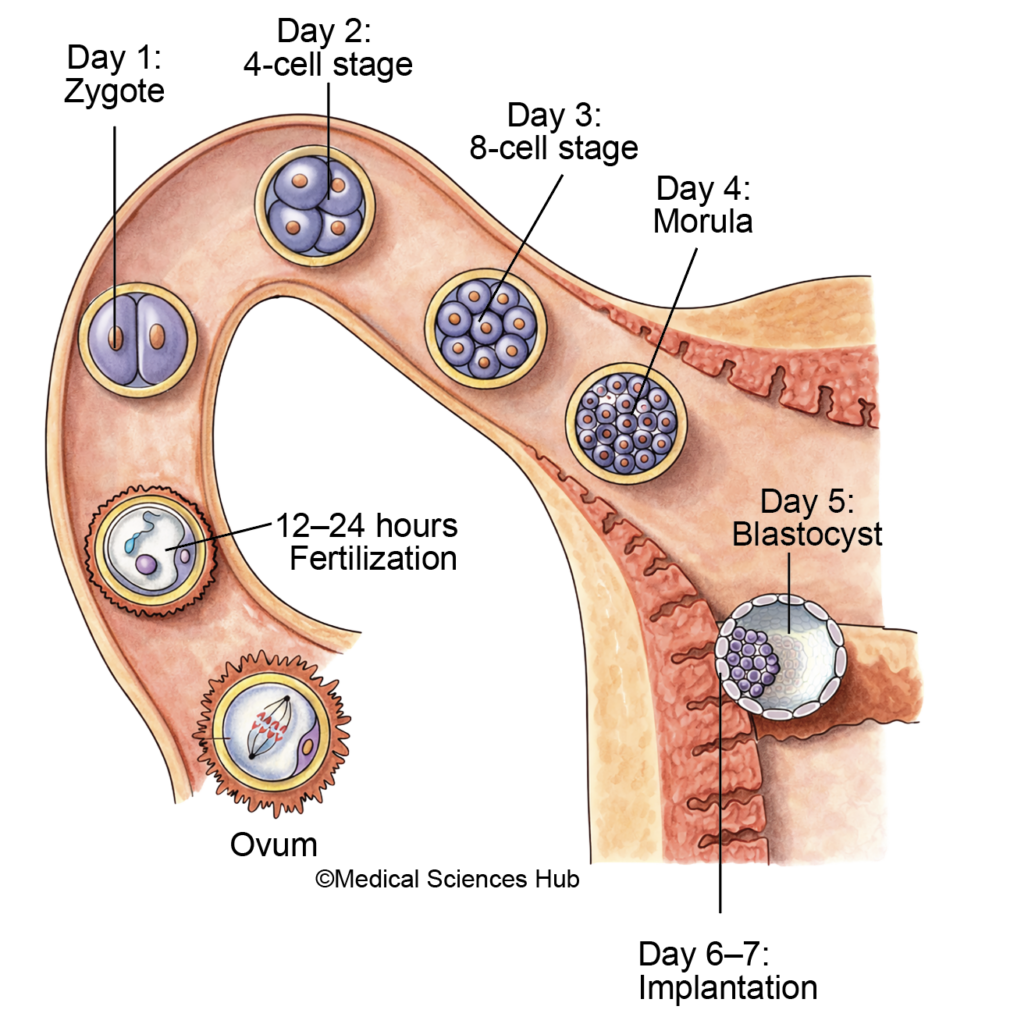
- The principal events during this period occur in a sequential manner (Figure 4.1):
- Day 0 — Spermatozoa surround the secondary oocyte in the ampulla of the uterine tube, and fertilization occurs, resulting in the formation of a zygote.
- Day 1 — The zygote undergoes its first mitotic division and reaches the 2-cell stage.
- Day 2 — Cleavage continues, producing a 4-cell stage embryo.
- Day 3 — Further mitotic divisions lead to the 8-cell stage.
- Day 4 — Compaction takes place, and a solid mass of cells called the morula is formed.
- Day 5 — A fluid-filled cavity develops within the morula, forming a blastocyst composed of an inner cell mass and an outer trophoblast.
- Day 6 — The blastocyst attaches to the endometrial epithelium, initiating implantation.
FERTILIZATION
- Definition: Fertilization is the union of two mature haploid gametes, the secondary oocyte and the spermatozoon, resulting in the formation of a single diploid cell called the zygote.
- Fertilization restores the diploid number of chromosomes and marks the beginning of a new individual.
- Fertilization is functionally opposite to meiosis, which produces haploid gametes. During fertilization, the genetic material from both parents combines to form a genetically unique, undifferentiated zygote.
- Usual site of fertilization – Ampulla of the fallopian tube.
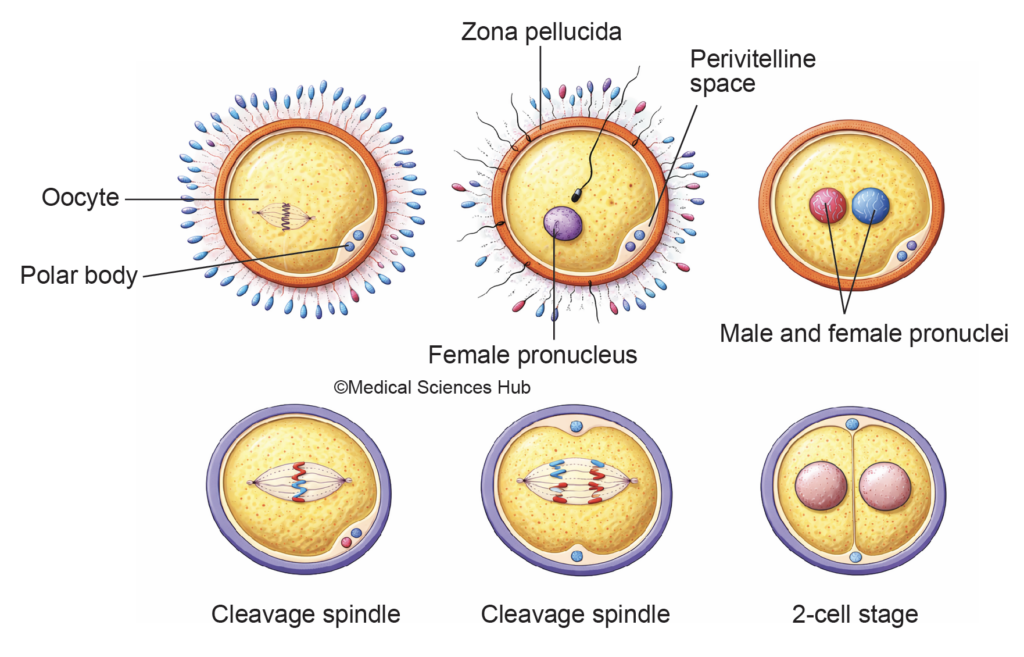
Stages of Fertilization
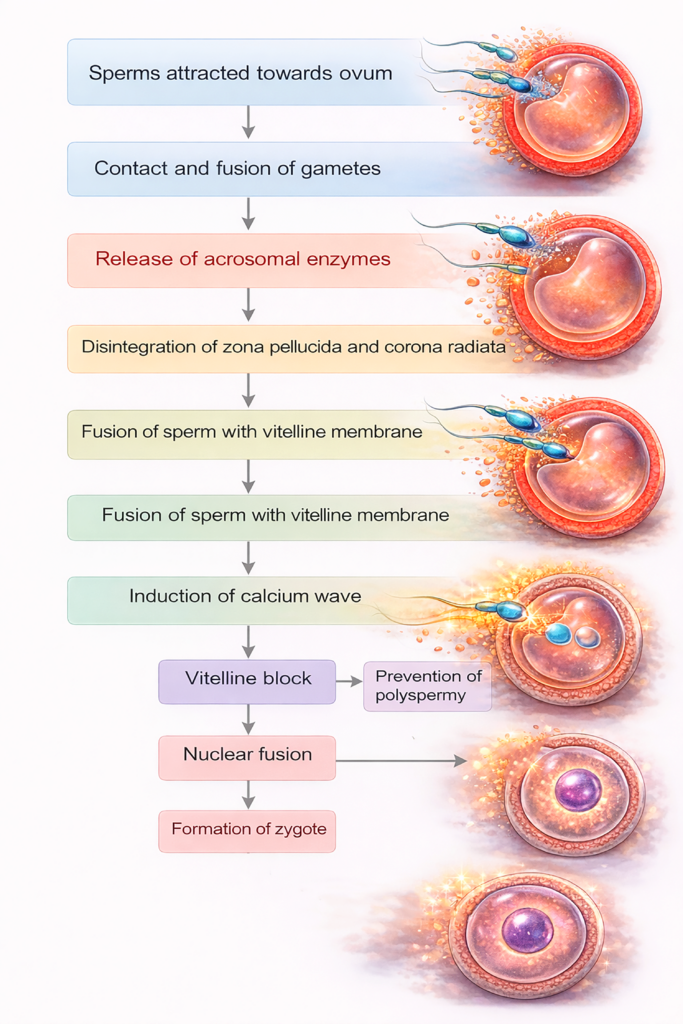
Fertilization should be studied in three basic steps events: approximation of gametes, contact and fusion of gametes and finally results of fertilization (Figure 4.2 and 4.2a, Flowchart 4.1).
- Approximation of gametes: This step involves transport of the spermatozoa through the female reproductive tract and the presence of the secondary oocyte within the uterine tube.
- Contact and fusion of gametes: This includes penetration of the corona radiata and zona pellucida by the spermatozoon, followed by fusion of the sperm and oocyte membranes.
- Results of fertilization: A series of cellular and molecular changes take place that constitute the outcome of fertilization, including completion of meiosis II in the oocyte, formation of male and female pronuclei, restoration of the diploid chromosome number, and formation of the zygote.
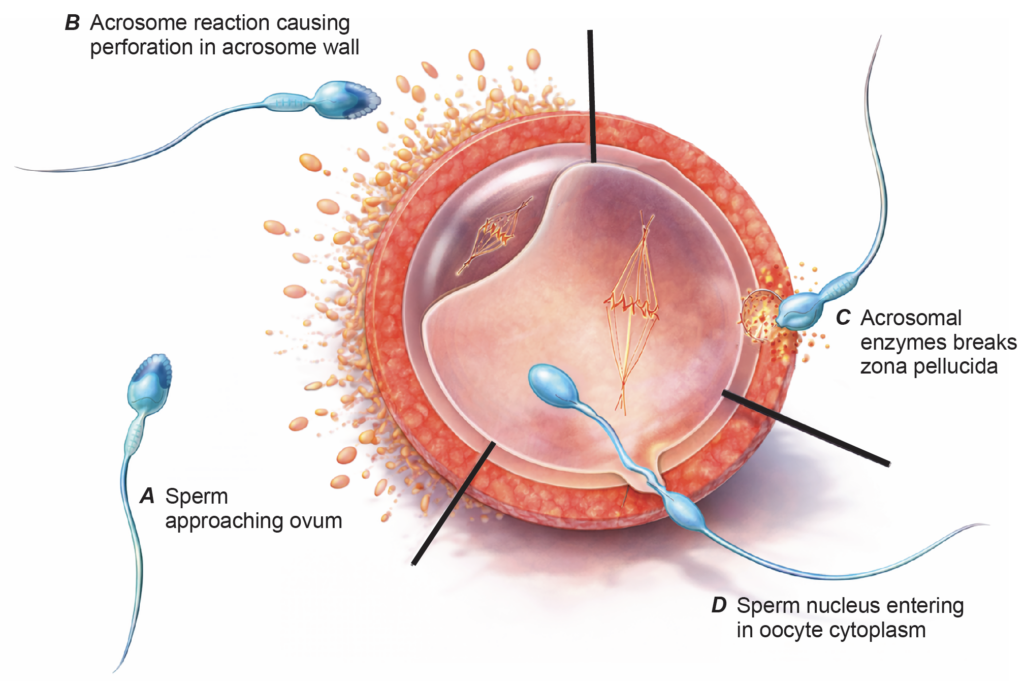
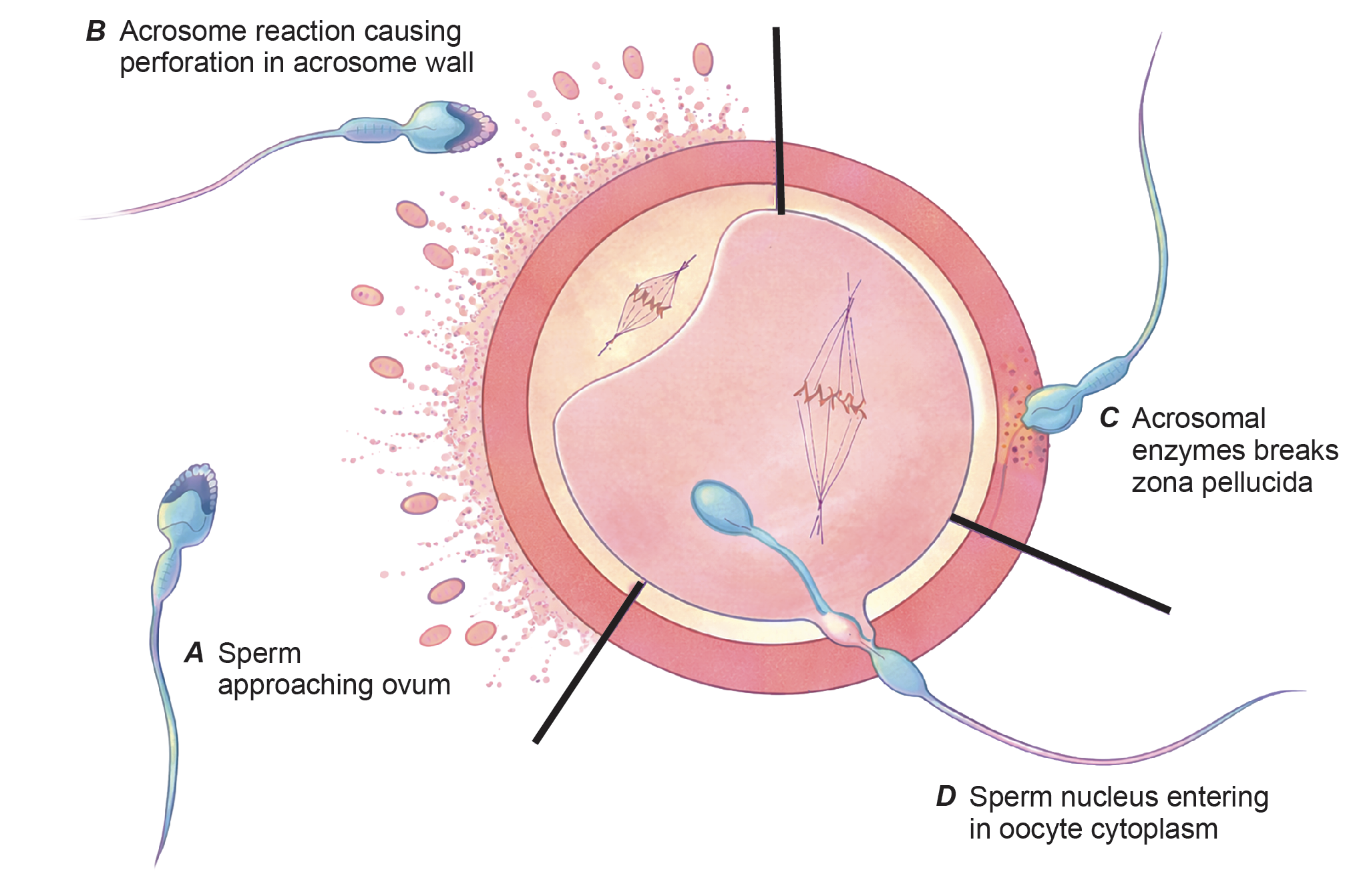
Figure 4.2a: Line diagram: Stages of fertilization (Click to see figure)
Approximation of Gametes
- This stage involves approximation of both spermatozoa and the secondary oocyte toward the ampulla of the uterine tube, which is the usual site of fertilization.
- Sperm transport within the female reproductive tract depends on several factors as follows:
- After ejaculation, semen liquefies within about 30 minutes due to fibrinolysin, allowing spermatozoa to become motile.
- Prostaglandins present in semen stimulate uterine contractions.
- Sexual intercourse also promotes oxytocin release from the posterior pituitary, which enhances uterine motility.
- Repeated uterine contractions facilitate upward movement of sperm into the uterine cavity and uterine tube.
- In addition, chemical signals from cells of the corona radiata guide sperm toward the oocyte.
- Although millions of sperm are deposited in the vagina, only about 1% enter the cervix, and approximately 300–500 reach the uterine tube.
- Transport from cervix to tube usually takes 2–7 hours. Spermatozoa remain viable in the female tract for 24–48 hours and may survive up to 4 days.
- Transport of ovum
- After ovulation, the secondary oocyte is guided into the fimbriated end of the uterine tube. Coordinated ciliary activity of the tubal epithelium and rhythmic contractions of the smooth muscle wall move it toward the ampulla.
- The sweeping action of the fimbriae assists in capturing the oocyte from the peritoneal cavity.
- In some cases, the oocyte may enter the contralateral uterine tube through transperitoneal migration.
- The oocyte usually reaches the ampulla within about 25 minutes after release. It remains viable for fertilization for approximately 12–24 hours.
Contact and Fusion of Gametes
- For fertilization to occur, the spermatozoon must cross three layers surrounding the secondary oocyte: the corona radiata, the zona pellucida, and the oocyte plasma membrane.
- During its passage through the female reproductive tract, the sperm undergoes capacitation. This is a functional maturation process in which glycoproteins and seminal plasma proteins are removed from the sperm head. These changes increase motility and prepare the sperm for binding and penetration. Capacitation usually requires about 7 hours.
- Penetration of the oocyte occurs in four stages.
Phase I: Acrosome reaction
The sperm binds to the zona pellucida, which triggers release of acrosomal enzymes such as hyaluronidase and acrosin. These enzymes help the sperm pass through the surrounding layers.
Phase II: Penetration of barriers
- Hyaluronidase disperses cells of the corona radiata.
- The sperm then binds to ZP3 receptors on the zona pellucida, and acrosin facilitates its passage through this layer.
- Fusion occurs between the sperm membrane and the oocyte plasma membrane through interaction of specific surface proteins. This phase takes about 30 minutes.
Phase III: Oocyte activation
- Fusion of the sperm with the oocyte membrane initiates a rise in intracellular calcium. This calcium wave causes completion of the second meiotic division, forming the female pronucleus and a second polar body.
- It also triggers release of cortical granules, which modify the zona pellucida and prevent entry of additional sperm, thereby blocking polyspermy.
Phase IV: Formation of the zygote
- The sperm nucleus enters the oocyte cytoplasm and forms the male pronucleus.
- The sperm mitochondria degenerate, so mitochondria in the zygote are of maternal origin.
- The male and female pronuclei replicate their DNA, their membranes break down, and the chromosomes align on a common mitotic spindle.
- True fusion of pronuclear membranes does not occur. Completion of the first mitotic division produces two diploid cells, marking formation of the zygote.
Results of Fertilization
- Fertilization triggers completion of the second meiotic division of the secondary oocyte, leading to formation of the female pronucleus and extrusion of the second polar body.
- Fertilization restores the diploid chromosome number. The male and female pronuclei, each containing 23 chromosomes, contribute to the formation of a zygote with 46 chromosomes.
- Chromosomal sex is established at the time of fertilization. An X-bearing sperm results in a 46,XX zygote, whereas a Y-bearing sperm produces a 46,XY zygote.
- Fertilization initiates cleavage. The zygote begins a series of mitotic divisions that mark the start of embryonic development.
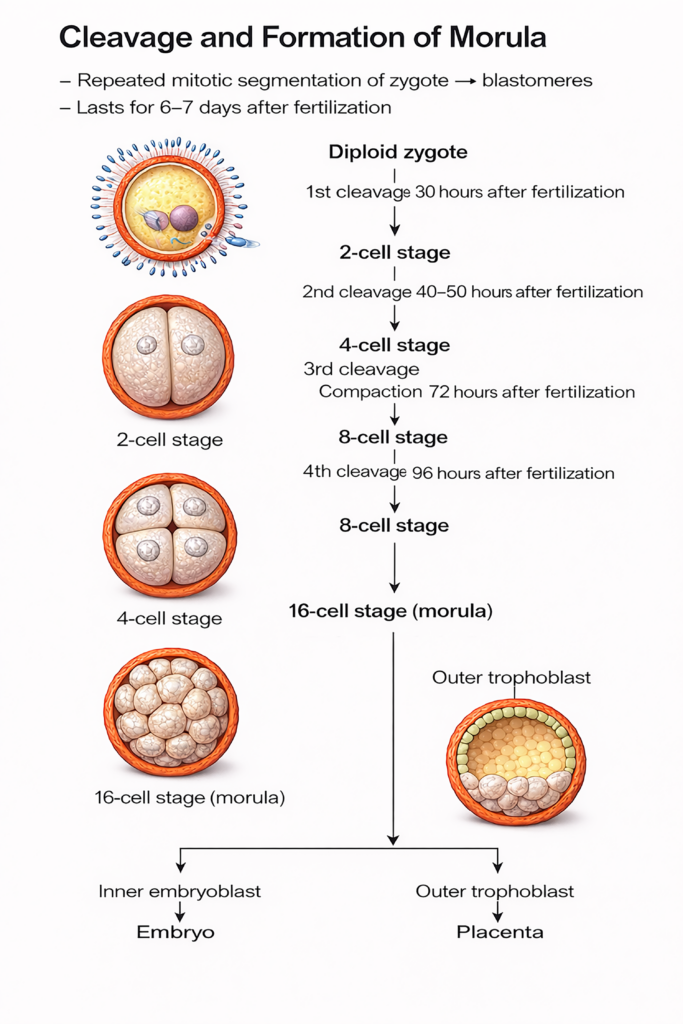
CLEAVAGE
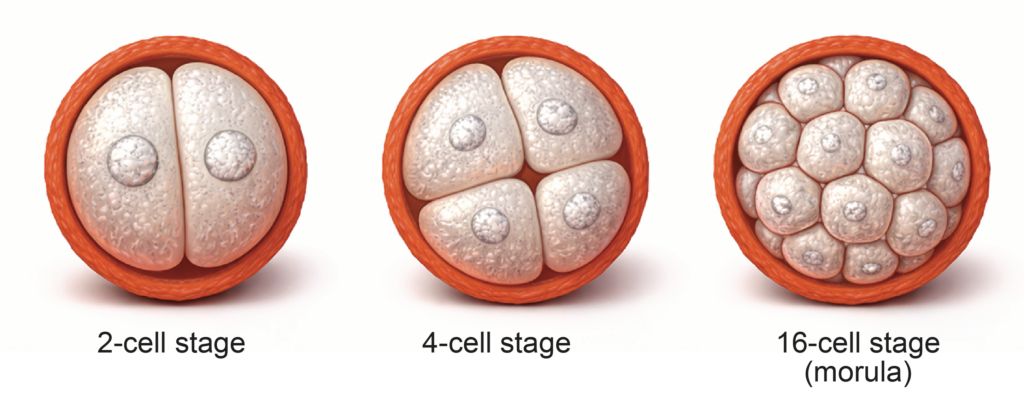
- Definition: Cleavage is a series of rapid mitotic divisions of the zygote that occur while it remains enclosed within the zona pellucida. These divisions produce progressively smaller cells known as blastomeres. During this process, the single-celled zygote divides into 2-cell, 4-cell, 8-cell stages and continues further without an overall increase in size (Figure 4.3).
- Duration: Cleavage begins soon after fertilization and continues for about 6 to 7 days, until implantation starts. As division proceeds, the cytoplasm is partitioned into smaller cells, leading to an increase in the nucleocytoplasmic ratio.
- Site: Cleavage starts in the ampulla of the uterine tube and continues as the developing conceptus moves toward the uterine cavity, where implantation subsequently occurs.
Events or Stages of Cleavage
- During cleavage, the zygote undergoes repeated mitotic divisions in which the cytoplasm is partitioned into progressively smaller blastomeres. The divisions may produce blastomeres of unequal size in the early stages. Larger blastomeres can enter the next mitotic cycle slightly earlier than smaller ones.
- The purpose of cleavage is to increase the number of cells without increasing the overall size of the conceptus, leading first to the formation of the morula and subsequently to the blastocyst.
Formation of morula
- The zygote undergoes successive mitotic divisions as it moves along the uterine tube.
- The first cleavage occurs about 24 to 30 hours after fertilization and produces a 2-cell stage (Figure 4.4, Flowchart 4.2).
- The second cleavage, at approximately 40 to 50 hours, results in a 4-cell stage.
- The third cleavage occurs around 66 hours and forms the 8-cell stage.
- After the 8-cell stage, compaction takes place. During this process, blastomeres increase their surface contact and form a closely packed cluster. The cells begin to differentiate into an inner cell mass and an outer cell layer.
- The fourth cleavage, at about 96 hours, produces a 16-cell stage.
- At this stage, the embryo resembles a mulberry and is called a morula (Figure 4.4).
- The morula consists of an inner cell mass, also known as the embryoblast, which gives rise to the embryo proper, and an outer cell layer called the trophoblast, which contributes to the fetal part of the placenta. The entire morula remains surrounded by the zona pellucida.
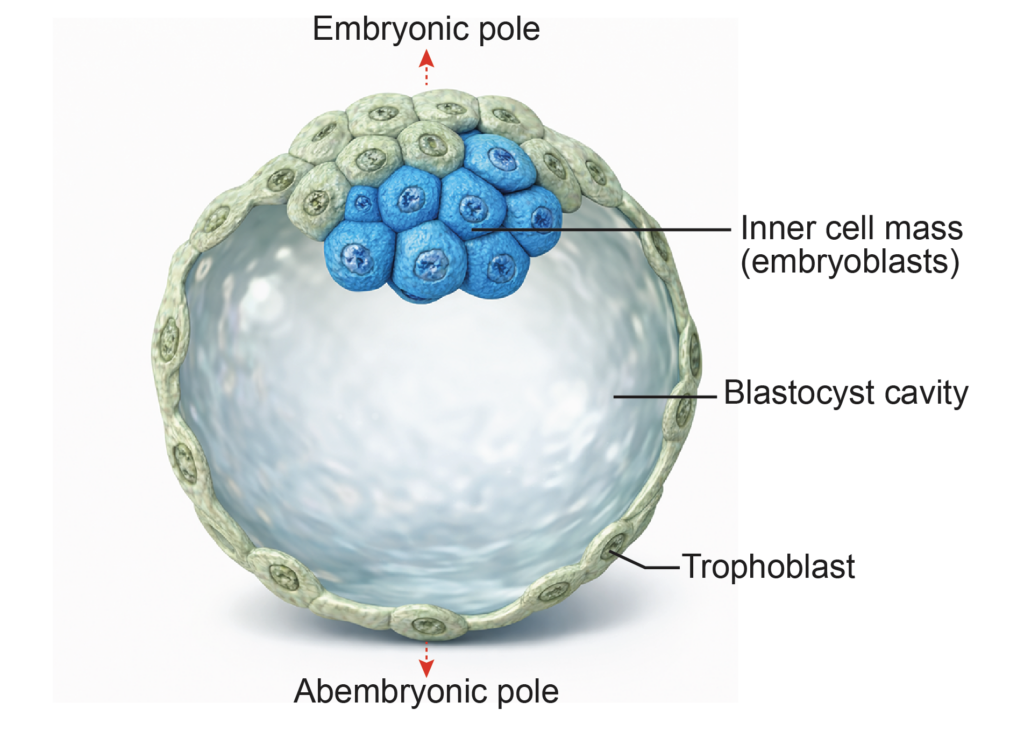
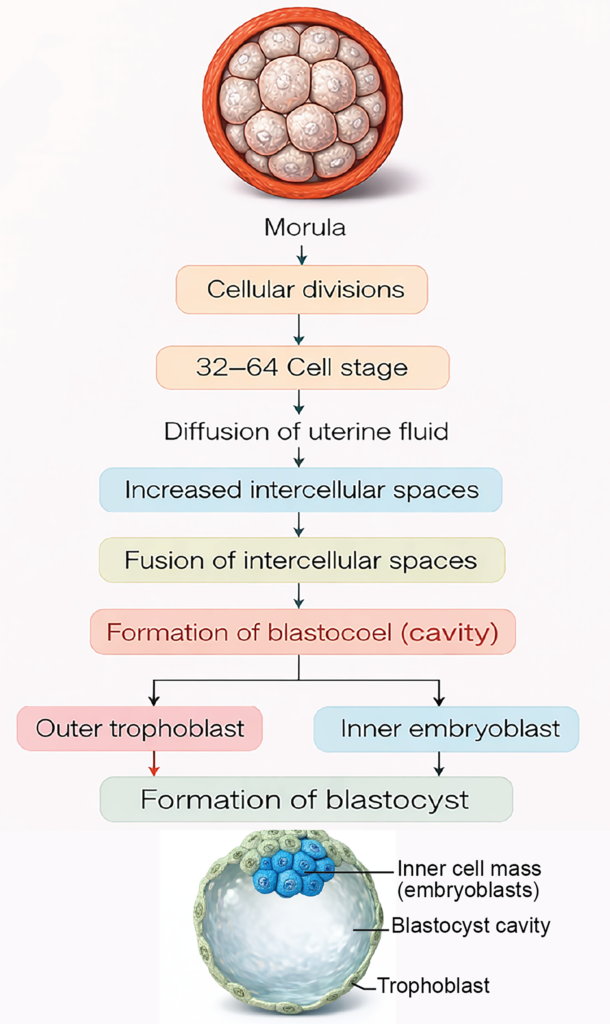
Formation of blastocyst
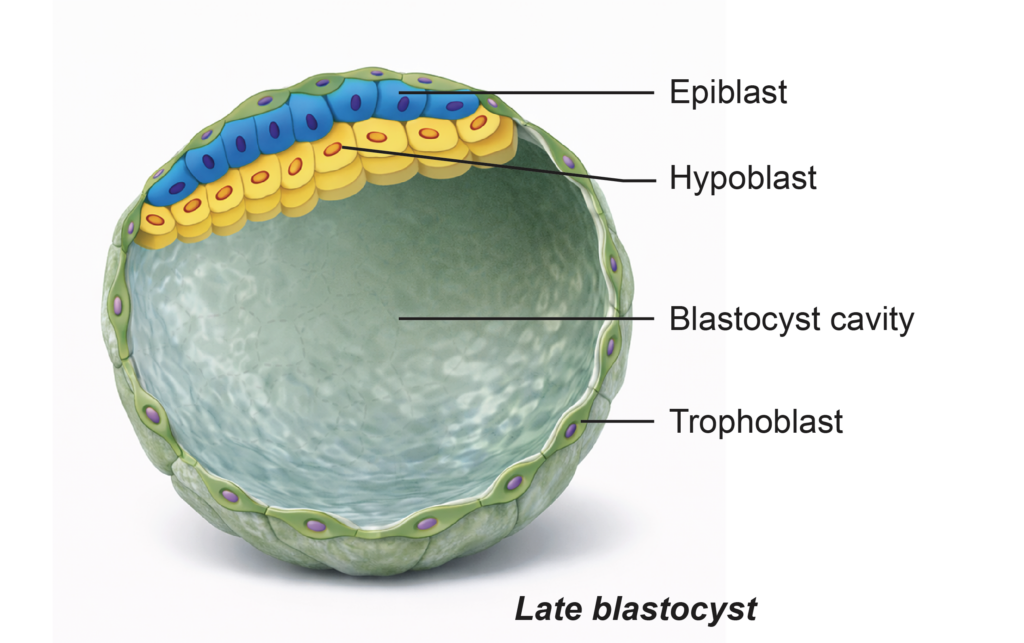
- The cells of the morula continue to divide and form a 32–64 cell stage. During this period, uterine fluid passes through the zona pellucida and accumulates between the cells. Small spaces appear within the morula, and these spaces gradually merge to create a single fluid-filled cavity called the blastocoel (Figure 4.5 and 4.6, Flowchart 4.3).
- As this cavity enlarges, the outer flattened cells form the trophoblast, while the inner group of cells becomes the embryoblast. The combination of trophoblast, embryoblast, and blastocoel constitutes the blastocyst.
- The region where the embryoblast is attached to the trophoblast is termed the embryonic pole, and the opposite side is the abembryonic pole. The trophoblast overlying the embryoblast is known as the polar trophoblast, and the remaining part is the mural trophoblast.
- During cleavage, the conceptus moves from the site of fertilization toward the uterine cavity. This transport is aided by ciliary activity and rhythmic contractions of the uterine tube. The developing embryo usually reaches the uterus about 4 to 5 days after fertilization, typically at the 32-cell stage.
- The embryoblast gives rise to the embryo proper. The trophoblast contributes to the formation of the placenta. The blastocoel later participates in formation of the yolk sac.
IMPLANTATION
- Definition: Implantation is the process by which the blastocyst attaches to and invades the endometrium of the uterus.
- Time
- Implantation usually begins on the 6th or 7th day after fertilization, when the embryo has reached the blastocyst stage.
- The process is generally completed by the 12th day after fertilization, which corresponds to approximately the 20th to 22nd day of a typical menstrual cycle.
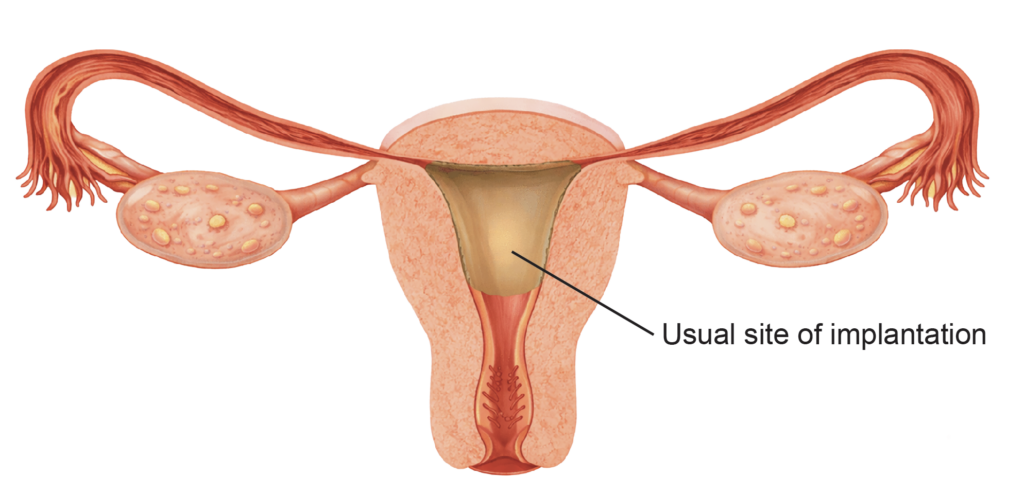
Site of Implantation
- Implantation usually takes place in the upper part of the body of the uterus, near the midline (Figure 4.7).
- It most often occurs on the posterior wall (about 55%) and less commonly on the anterior wall (about 45%).
- In humans, the blastocyst becomes completely embedded within the endometrium; this type is known as interstitial implantation.
Process of implantation
- The blastocyst undergoes hatching. The zona pellucida prevents attachment to the uterine lining, so it must degenerate before implantation can occur. Around the sixth day after fertilization, enzymatic activity from the trophoblast leads to breakdown of the zona pellucida (Figure 4.8).
- Next, the trophoblast adheres to the endometrial epithelium. Attachment usually occurs at the embryonic pole. This adhesion is mediated by interactions between surface molecules on trophoblastic cells and specific receptors on the uterine epithelium. Initial contact generally occurs 5 to 7 days after fertilization, shortly before invasion begins.
- Following adhesion, the trophoblast proliferates and secretes proteolytic enzymes that digest the endometrial tissue. This allows the blastocyst to penetrate deeper into the endometrium until it becomes completely embedded.
- Finally, the surface defect created by penetration is sealed. By about the ninth day after fertilization, the endometrial epithelium regenerates and a fibrin plug temporarily closes the site of entry.
CLINICAL EMBRYOLOGY
- Abnormal Implantation
- If the conceptus implants outside the normal site in the upper part of the uterine body, the condition is termed ectopic implantation and results in an ectopic pregnancy.
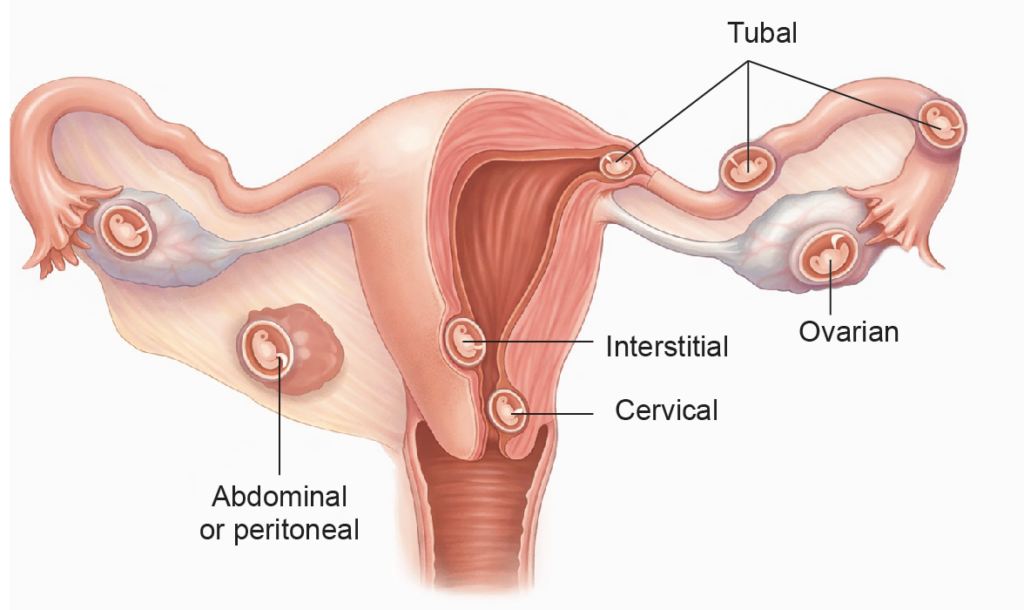
- Ectopic implantation is classified according to its location as follows (Figure 4.9):
- Abnormal uterine implantation:
- In placenta previa, the placenta develops in the lower uterine segment and partially or completely covers the internal os.
- In intramural implantation, the conceptus is embedded within the myometrium.
- In placenta previa, the placenta develops in the lower uterine segment and partially or completely covers the internal os.
- Tubal implantation: Implantation occurs within the uterine tube. This is the most common form of extrauterine pregnancy and accounts for about 95% of cases.
- Abdominal implantation: This is uncommon and may occur on structures such as the ovary or peritoneal surfaces, including the mesentery.
- Abnormal uterine implantation:
- Many ectopic pregnancies are anembryonic. Patients often present with acute lower abdominal pain, sometimes associated with vaginal spotting. Early diagnosis and management are essential to prevent serious complications, including hemorrhage.
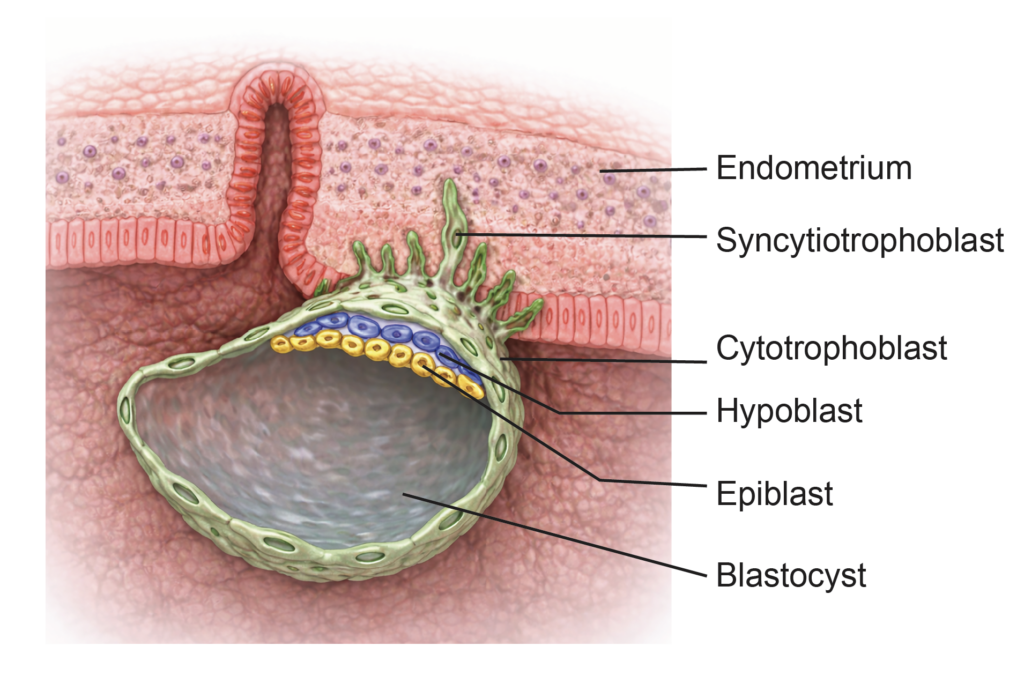
CHANGES IN TROPHOBLAST DURING IMPLANTATION
- After the blastocyst attaches to the endometrium at the embryonic pole, the trophoblast begins to differentiate, usually between the 6th and 8th day after fertilization.
- Two distinct layers are formed.
- The inner layer is the cytotrophoblast, which consists of mononuclear cells with clear cell boundaries and mitotic activity.
- The outer layer is the syncytiotrophoblast, which is a multinucleated mass formed by fusion of trophoblastic cells and lacks distinct cell membranes.
- The syncytiotrophoblast extends finger-like projections into the endometrium. These projections facilitate invasion of the uterine tissue and enable the blastocyst to become embedded within the endometrium.
Important Questions
- Write a short note on fertilization.
- List the effects (consequences or results) of fertilization.
- Write a short note on functions of zona pellucida.
- Write a short note on cleavage.
- Write a short note on morula.
- Write a short note on formation of blastocyst.
- What is reverse cleavage?
- Write a short note on implantation.
- List the abnormal sites of implantation.
- Write a short note on methods of contraception.
