Competencies
- AN77.1: Describe the uterine changes occurring during the menstrual cycle.
- AN77.2: Describe the synchrony between the ovarian and menstrual cycles.
INTRODUCTION
- The menstrual cycle is a series of cyclic changes occurring in the ovaries and uterus during the reproductive years. These changes prepare the female reproductive system for fertilization and implantation. The average cycle length is about 28 days.
- The female reproductive system consists of two ovaries, two uterine tubes, the uterus, the vagina, and the external genitalia. The reproductive period extends from puberty to menopause.
- Puberty is the stage when secondary sexual characteristics appear, and reproductive capacity begins. It usually occurs between 10 and 14 years of age.
- Menopause is defined as the permanent cessation of menstruation for 12 consecutive months. It marks the end of natural reproductive capacity. It commonly occurs between 45 and 55 years of age.
- During the reproductive years, cyclic changes occur approximately every month in the ovaries and uterus. These changes are regulated by the hypothalamo–pituitary–ovarian axis through coordinated hormonal secretion.
- The cyclic changes are classified into:
- Ovarian cycle: It includes development and maturation of ovarian follicles, ovulation, formation of corpus luteum, and secretion of estrogen and progesterone.
- Uterine (menstrual) cycle: It involves cyclic changes in the endometrium for implantation. If fertilization does not occur, the functional layer of the endometrium is shed as menstruation.
- The ovarian cycle and ovulation are described separately. The present section focuses on the uterine or menstrual cycle.
| Ovarian Cycle | Uterine Cycle |
|---|---|
| Follicular phase | Menstrual phase |
| Ovulation | Proliferative phase |
| Luteal phase | Secretory phase |
MENSTRUAL CYCLE
- The menstrual cycle consists of regular, cyclic changes in the uterus during the reproductive period, beginning at puberty and ending at menopause. Menstruation is the periodic discharge of blood and shed endometrial tissue through the vagina. It occurs when fertilization and implantation do not take place in a given cycle.
Duration
- Each menstrual cycle begins on the first day of menstrual bleeding and ends on the day before the next menstrual bleeding starts. The length of the cycle varies among individuals. In the same individual, the duration may also show minor variation.
- The average cycle length is 28 days. The normal range is 21 to 35 days in adults.
- Menstrual cycles are temporarily absent during pregnancy. They may also be suppressed during lactation due to hormonal changes associated with breastfeeding.
PHASES OF MENSTRUAL CYCLE
- The menstrual cycle is described in four phases:
- Follicular phase
- Proliferative phase
- Secretory phase
- Menstrual phase
- The follicular phase corresponds to the ovarian changes and includes the early menstrual phase followed by the proliferative phase of the endometrium. The secretory phase corresponds to the luteal phase of the ovary.
- Clinically, the cycle is divided into two main parts: the follicular phase and the luteal phase. Ovulation occurs between these two phases and marks the transition from the follicular to the luteal phase.
Follicular Phase (Preovulatory)
- The developing ovarian follicles secrete estrogen. This hormone regulates cyclic changes in the endometrium. Therefore, the first half of the menstrual cycle is called the follicular phase. It extends from the first day of menstruation until ovulation.
- The follicular phase includes two components:
i. Menstrual phase
ii. Proliferative phase
- The follicular phase includes two components:
- In the initial days, the functional layer of the endometrium, including the stratum compactum and stratum spongiosum, is shed. This shedding produces menstrual bleeding that usually lasts 3 to 5 days. This period is termed the menstrual phase.
- After menstruation, the endometrium regenerates and increases in thickness under the influence of estrogen. This period is known as the proliferative phase.
Luteal/Secretory Phase (Postovulatory)
- After ovulation, the corpus luteum develops from the ruptured follicle and secretes progesterone. This hormone regulates changes in the endometrium. Therefore, this part of the cycle is called the luteal phase or progestational phase.
- During the luteal phase, the endometrium becomes thick, vascular, and glandular. The endometrial glands show increased secretory activity. Hence, this period is also termed the secretory phase.
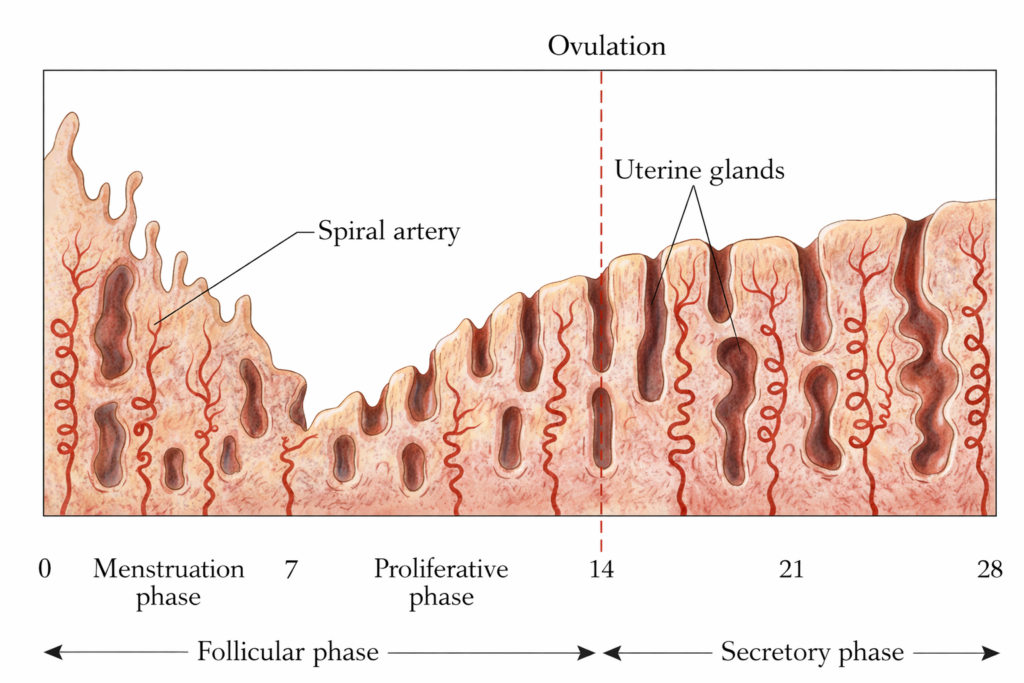
UTERINE CHANGES IN MENSTRUAL CYCLE
- During each menstrual cycle, both the ovary and the uterus undergo coordinated cyclic changes. The ovarian changes include follicular development, ovulation, and formation of the corpus luteum.
- The uterine changes involve sequential alterations in the endometrium during the menstrual, proliferative, and secretory phases. These changes correspond to specific phases of the cycle and are regulated by hormonal interactions.
Changes in Follicular Phase
Changes in Menstrual phase
- At the end of the previous cycle, the corpus luteum degenerates. This leads to a fall in progesterone and estrogen levels. The decrease in these hormones causes constriction of spiral arteries.
- Reduced blood flow leads to ischemia and necrosis of the functional layer of the endometrium, including the stratum compactum and stratum spongiosum. These layers form the superficial two-thirds of the endometrium. The necrotic tissue is shed as menstrual bleeding.
- The average duration is 3 to 5 days.
Changes in Proliferative phase (oestrogenic phase)
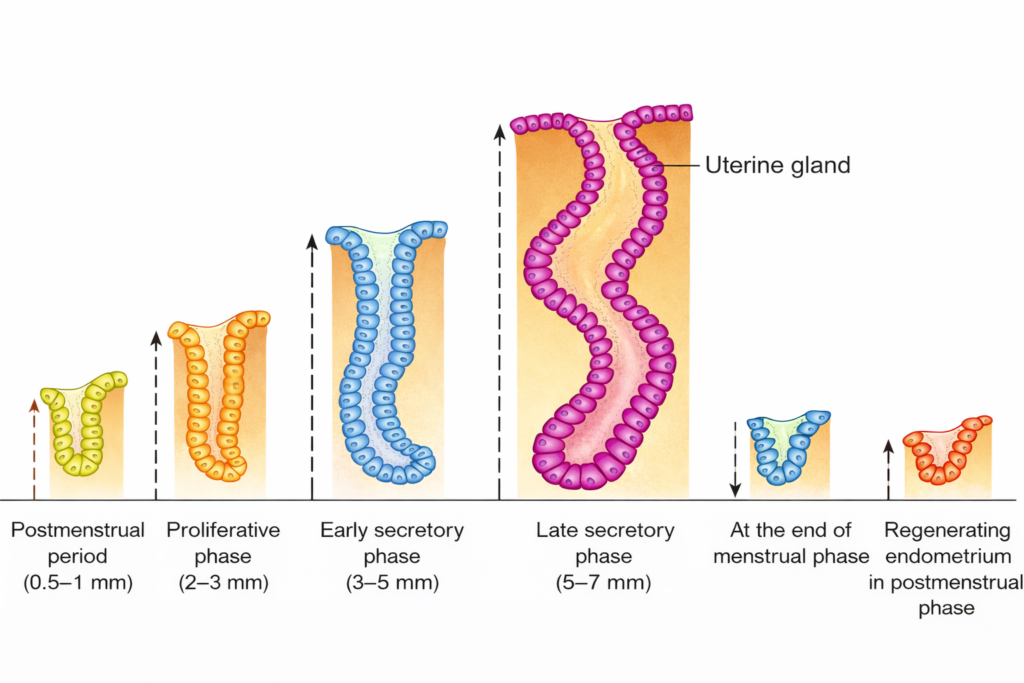
- From about the 5th day onward, estrogen stimulates regeneration of the endometrium from the stratum basale. The endometrium increases in thickness due to cell proliferation and enlargement.
- The uterine glands become straight, elongated, and widely spaced. They show minimal secretion. Spiral arteries lengthen and increase in number, improving vascular supply.
- Estrogen increases the volume, alkalinity, and elasticity of cervical mucus, which facilitates sperm passage through the cervix.
Changes in Luteal/Secretory Phase
- In the luteal phase, the corpus luteum secretes high levels of progesterone. This hormone prepares the endometrium for possible implantation.
- Glandular changes
- The uterine glands enlarge and become highly coiled and tortuous. The epithelial cells accumulate glycogen. The glands secrete a carbohydrate-rich fluid that can support an early embryo.
- Stromal and vascular changes
- The spiral arteries lengthen and become more tortuous. Endometrial vascularity increases.
- The stroma becomes edematous due to fluid accumulation. Stromal cells enlarge and store glycogen and lipid droplets. This transformation is known as the decidual reaction.
- If implantation does not occur, the corpus luteum regresses. Progesterone levels fall. Constriction of spiral arteries leads to ischemia and focal necrosis of the functional layer. These changes result in the onset of menstruation.
- Cervical mucus changes
- Progesterone makes the cervical mucus thick and less elastic. This reduces the passage of sperm through the cervix.
- Glandular changes
OVARIAN CHANGES IN MENSTRUAL CYCLe
Changes in Follicular Phase
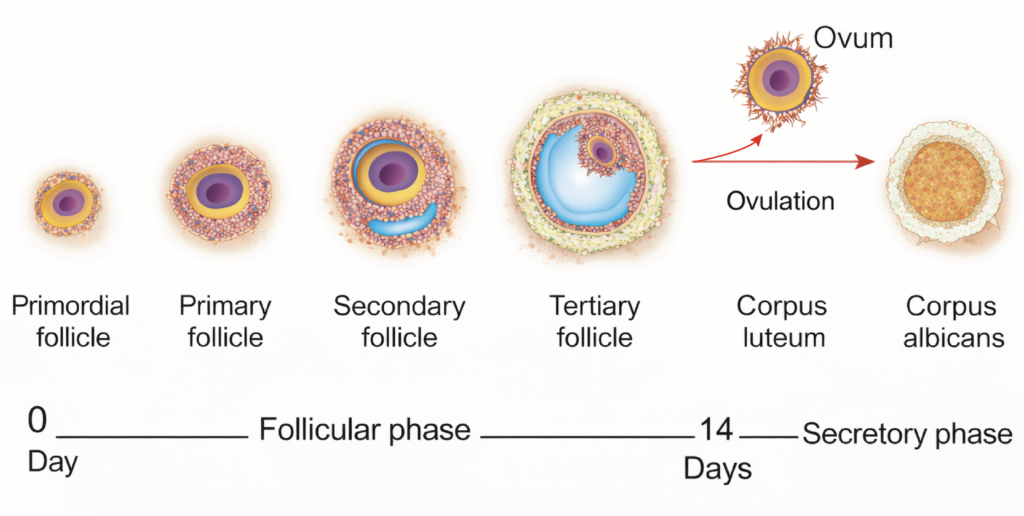
- During each ovarian cycle, several follicles begin to develop. Usually, only one follicle becomes dominant and reaches the stage of a mature Graafian follicle.
- The primary oocyte increases in size and is surrounded by follicular cells. These structures progress through primary, secondary, and tertiary follicular stages.
- Fluid called liquor folliculi accumulates within the follicle. This fluid separates the granulosa cells into an outer stratum granulosum and an inner group of cells surrounding the oocyte, called the cumulus oophorus.
- The surrounding stromal cells differentiate into the theca interna and theca externa. Granulosa cells produce estrogen, which regulates endometrial changes. Shortly before ovulation, the primary oocyte completes the first meiotic division to form a secondary oocyte and a first polar body.
- At the end of the follicular phase, the mature follicle ruptures and releases the secondary oocyte.
Changes in Luteal (Progestational) Phase
- The luteal phase begins immediately after ovulation. After rupture of the mature follicle, the follicular cavity fills with blood. This structure is called the corpus hemorrhagicum.
- The granulosa and theca cells enlarge and accumulate a yellow pigment known as lutein. This transformation is called luteinization. The resulting structure is the corpus luteum. It secretes progesterone and a smaller amount of estrogen.
- If fertilization does not occur, the corpus luteum remains functional for about 14 days and then regresses by the end of the cycle.
- If pregnancy occurs, the corpus luteum of pregnancy persists for approximately 10 to 12 weeks and maintains progesterone secretion.
- Degeneration of the corpus luteum is termed luteolysis. It is gradually replaced by fibrous scar tissue called the corpus albicans..
HORMONAL SYNCHRONIZATION IN MENSTRUAL AND OVARIAN CYCLES
- The menstrual cycle is regulated by the hypothalamo–pituitary–ovarian axis. The hypothalamus secretes gonadotropin-releasing hormone.
- This hormone stimulates the anterior pituitary to release follicle-stimulating hormone and luteinizing hormone. FSH and LH act on the ovaries. The ovaries produce estrogen and progesterone in response to these signals.
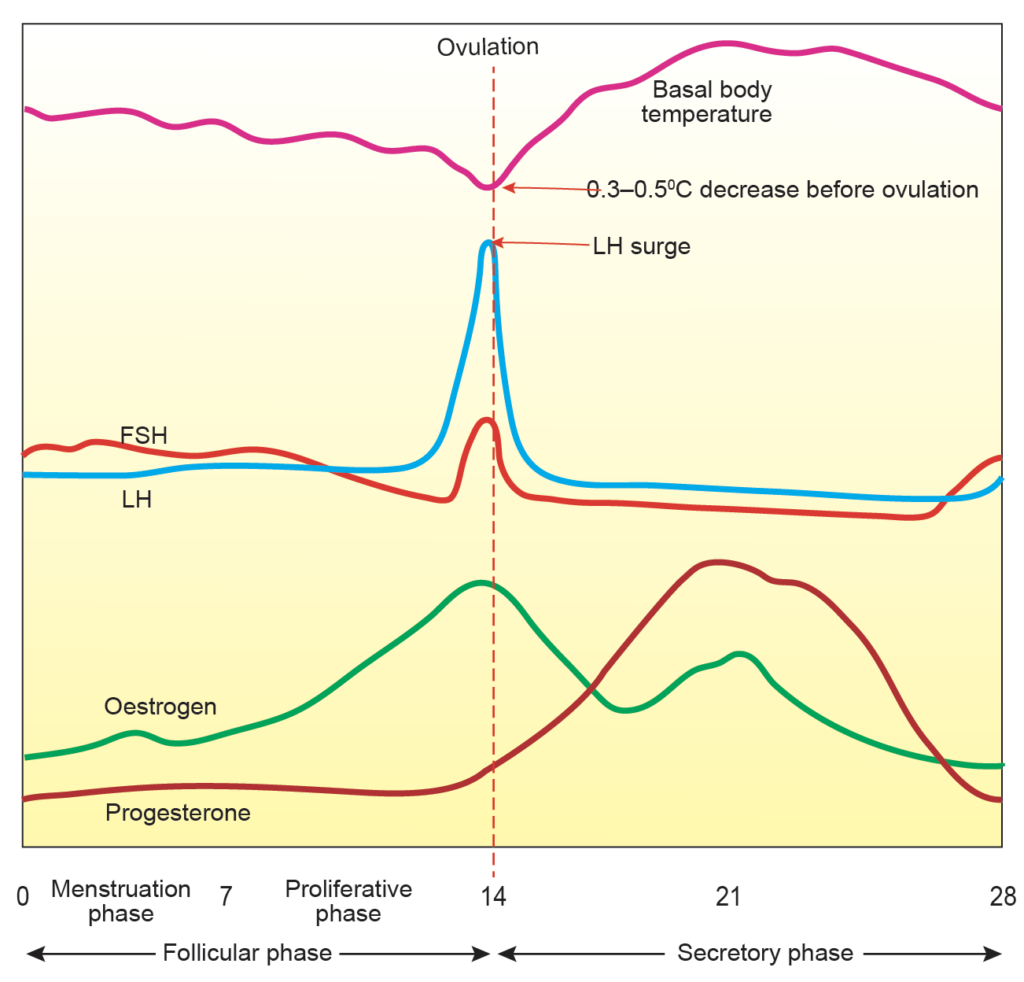
Estrogen
- Estrogen regulates endometrial proliferation and maintains secondary sexual characteristics. Its level rises during follicular development.
- A marked increase occurs about 48 hours before ovulation and induces the LH surge. After ovulation, estrogen declines briefly. It rises again during the mid-luteal phase due to corpus luteum activity.
Progesterone
- Progesterone is secreted mainly by the corpus luteum. Its level is low during the proliferative phase. It increases after ovulation and peaks about 4 to 5 days later.
- It declines at the end of the luteal phase if the corpus luteum regresses.
Luteinizing Hormone
- LH levels increase sharply about 34 to 36 hours before ovulation. This surge is triggered by sustained high estrogen levels.
- LH promotes prostaglandin production, increases follicular blood flow, enhances intrafollicular pressure, and stimulates proteolytic activity. These changes cause rupture of the follicle and release of the secondary oocyte.
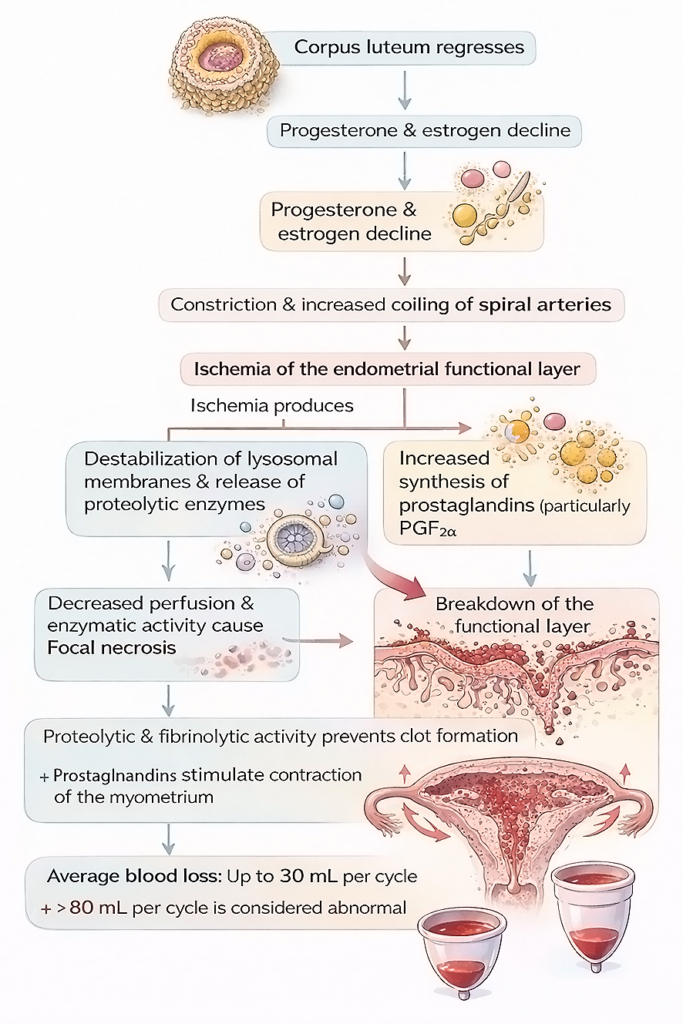
MECHANISM OF MENSTRUAL BLEEDING
- In the absence of pregnancy, the corpus luteum regresses. Progesterone and estrogen levels decline.
- The fall in steroid hormones causes constriction and increased coiling of spiral arteries.
- Reduced blood flow leads to ischemia of the functional layer of the endometrium.
- Ischemia produces the following effects:
- Destabilization of lysosomal membranes and release of proteolytic enzymes.
- Increased synthesis of prostaglandins, especially PGF₂α.
- Decreased perfusion and enzymatic activity cause focal necrosis. These areas enlarge and merge, resulting in breakdown of the functional layer.
- Proteolytic and fibrinolytic activity prevents clot formation in menstrual blood.
- Prostaglandins stimulate contraction of the myometrium. These contractions help expel the shed endometrial tissue.
- The average menstrual blood loss is up to 30 mL per cycle. Blood loss greater than 80 mL per cycle is considered abnormal.
CLINICAL EMBRYOLOGY
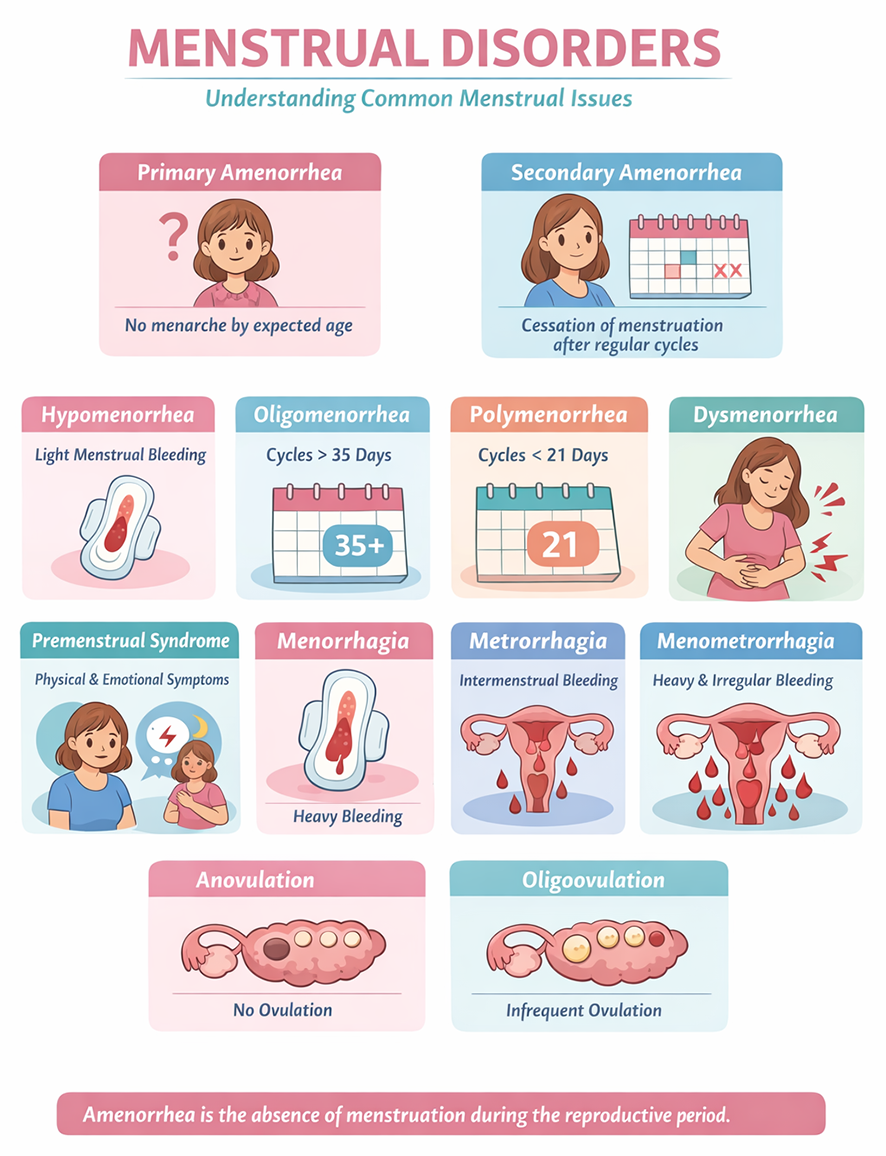
- Disorders Of Menstrual Cycle
- Menstrual disorders can be classified into four groups.
- Disorders of menstrual flow include amenorrhea, hypomenorrhea, and oligomenorrhea.
- Pain-related disorders include dysmenorrhea and premenstrual syndrome.
- Disorders of timing include menorrhagia, metrorrhagia, and menometrorrhagia.
- Disorders of ovulation include anovulation and oligoovulation.
- Menstrual disorders can be classified into four groups.
- Related terms
- Amenorrhea is the absence of menstruation during the reproductive period.
- Primary amenorrhea refers to failure to attain menarche by the expected age.
- Secondary amenorrhea is the cessation of menstruation in a woman who previously had regular cycles.
- Hypomenorrhea is abnormally light menstrual bleeding.
- Oligomenorrhea is infrequent menstruation with cycles longer than 35 days.
- Polymenorrhea is frequent menstruation with cycles shorter than 21 days.
- Dysmenorrhea is painful menstruation associated with uterine contractions.
- Premenstrual syndrome consists of physical and psychological symptoms occurring in the late luteal phase and resolving after onset of menstruation.
- Menorrhagia is excessive menstrual blood loss at regular intervals.
- Metrorrhagia is irregular uterine bleeding between cycles.
- Menometrorrhagia is heavy bleeding at irregular and frequent intervals.
- Anovulation is the absence of ovulation.
- Oligoovulation is infrequent or irregular ovulation.
Important Questions
- Write a short note on the phases of the menstrual cycle.
- Write a short note on the endometrium.
- Write a short note on uterine or endometrial changes in the menstrual cycle.
- Write a short note on the mechanism of menstrual bleeding.
- Write a short note on the hormonal control of the menstrual cycle.
- List the disorders of the menstrual cycle.
- Define amenorrhea, oligomenorrhea, dysmenorrhea, menorrhagia and anovulation.
