Competencies
- AN43.4: Describe the development and developmental basis of congenital anomalies of face, palate, tongue, branchial apparatus, pituitary gland, thyroid gland, eye.
INTRODUCTION
- The pharynx is a muscular tubular structure located posterior to the nasal and oral cavities. It develops from the cranial part of the foregut and later serves as a common pathway for both the respiratory and digestive systems.
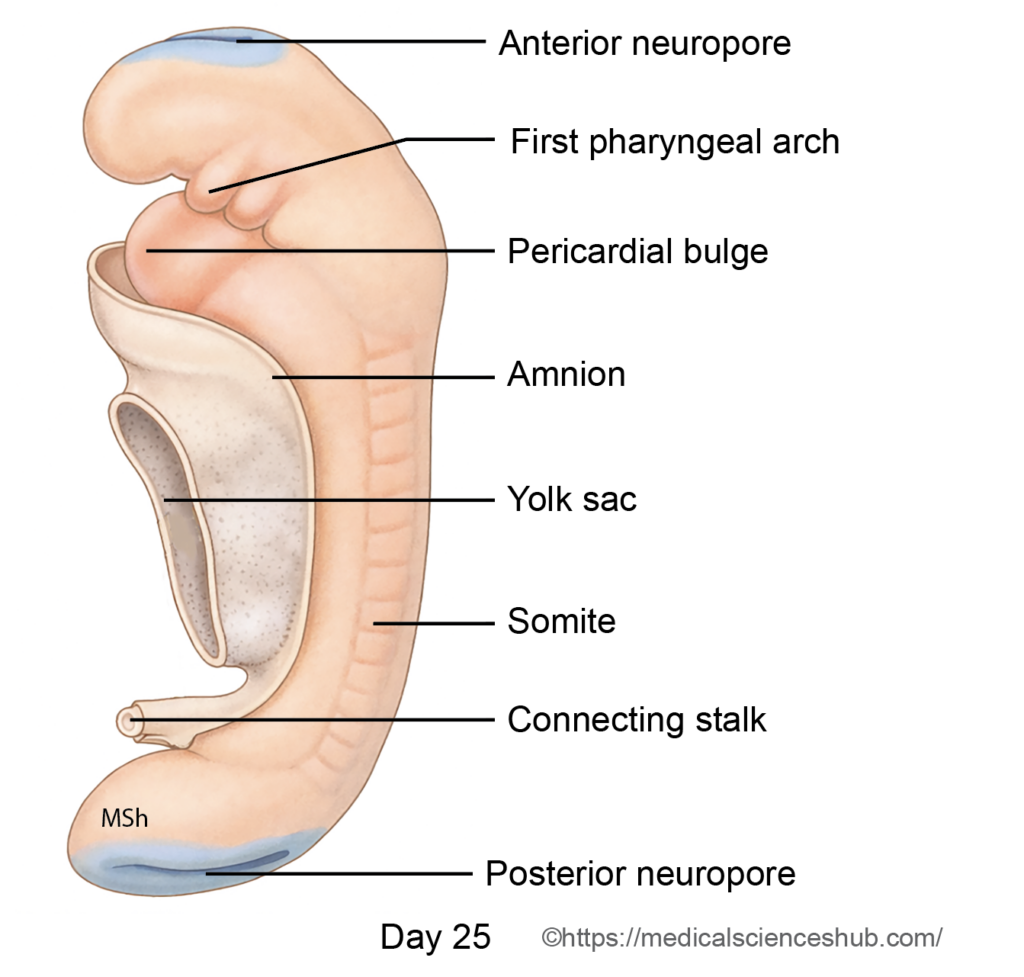
- During embryonic folding, part of the yolk sac is incorporated into the embryo to form the foregut. Rapid expansion of the forebrain vesicle positions the buccopharyngeal membrane within a surface depression called the stomodeum, located cranial to the pericardial bulge. The primitive pharynx lies dorsal and slightly caudal to the stomodeum and is bounded by a roof, floor, and paired lateral walls.
- Its early anatomical relations are as follows:
- Cranial: Forebrain
- Ventral (floor): Stomodeum, pericardial bulge, and septum transversum
- Dorsal (roof): Notochord and hindbrain vesicle
- Lateral: Splanchnopleuric mesoderm covered by surface ectoderm
- Initially, a distinct neck region is absent. As mesoderm proliferates between the stomodeum and pericardial bulge, segmental thickenings appear beneath the ectoderm. These paired elevations grow ventrally and fuse in the midline to form curved bar-like structures known as the pharyngeal (branchial) arches.
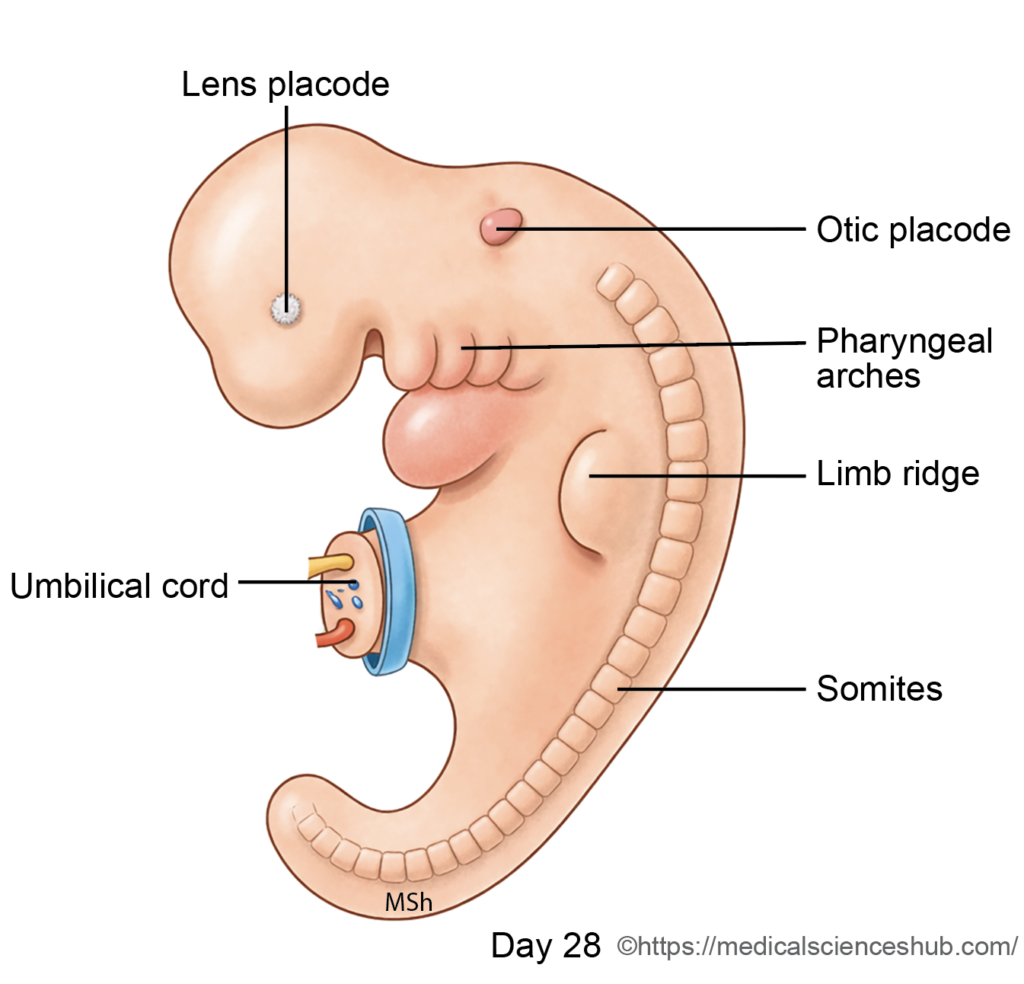
- Pharyngeal arches develop during the 4th and 5th weeks of development. Six arches develop sequentially; however, the fifth arch is rudimentary and regresses, resulting in five definitive arches. Internally, the endoderm of the primitive pharynx forms lateral outpocketings between adjacent arches called pharyngeal pouches. Externally, corresponding ectodermal indentations known as pharyngeal clefts (grooves) appear.
- The coordinated development of the arches, pouches, and clefts establishes the structural framework for formation of the head and neck.
Pharyngeal Apparatus
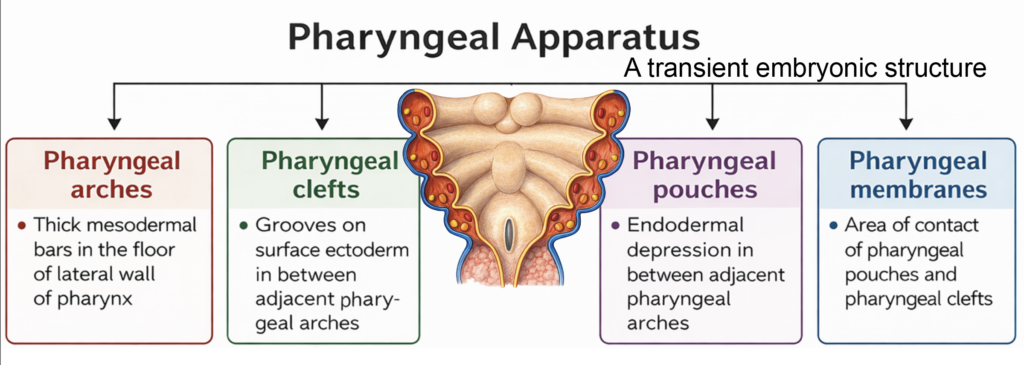
- The pharyngeal apparatus is a transient embryonic structure that forms the foundation of the head and neck. It consists of three principal components: pharyngeal arches, pharyngeal pouches, and pharyngeal clefts (grooves).
Components
- Pharyngeal Arches
The pharyngeal arches are paired mesenchymal swellings located in the floor and lateral walls of the primitive pharynx. They are composed of mesoderm and migrating neural crest cells and give rise to specific skeletal, muscular, vascular, and neural elements. - Pharyngeal Clefts (Grooves)
These are ectoderm-lined surface depressions situated between adjacent arches on the external aspect of the embryo. - Pharyngeal Pouches
The pharyngeal pouches are endoderm-lined outpocketings that develop between adjacent arches along the internal wall of the primitive pharynx. - At sites where a pharyngeal pouch contacts a corresponding cleft, a thin pharyngeal membrane is formed. This membrane consists of ectoderm, endoderm, and an intervening layer of mesenchyme. The tympanic membrane develops from the first pharyngeal membrane and represents derivatives of all three germ layers.
- In aquatic vertebrates, these membranes break down to create gill slits for respiration. In humans, they do not rupture. Instead, intervening mesenchyme contributes to the fibroareolar tissue of the neck.
Developmental Timeline
- The pharyngeal arches appear during the 4th and 5th weeks of development.
- By approximately day 22, the first and second arches are visible.
- By the end of the 5th week (around day 29), four well-defined arches are present.
- Although six arches form in sequence, the fifth is rudimentary and regresses.
- By the fourth week, the buccopharyngeal membrane ruptures, establishing communication between the foregut and the amniotic cavity, marking an important step in early digestive tract development.
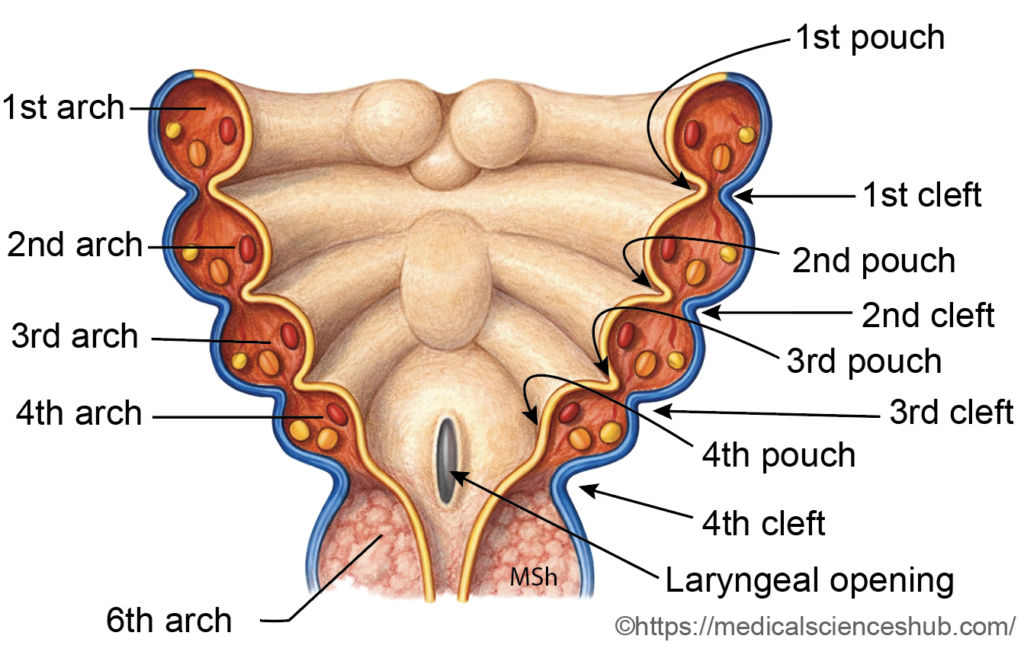
Figure 9.3a: Line diagram: Pharyngeal apparatus (Click to see figure)

PHARYNGEAL ARCHES
Definition
- The pharyngeal arches are paired, horseshoe-shaped mesenchymal bars located in the lateral walls and floor of the primitive pharynx. They form a major structural framework for the developing head and neck.
- Six arches develop in sequence during early embryogenesis. However, the fifth arch is rudimentary and regresses, leaving five functional arches.
Structural Components
- Each arch contains a core of splanchnopleuric mesoderm infiltrated by migrating neural crest cells. These neural crest cells give rise to most of the skeletal elements and connective tissue of the face and neck, including the viscerocranium (facial skeleton).
- The mesodermal component of each arch differentiates into:
- A specific muscle group
- An associated pharyngeal arch artery
- Each arch is also supplied by a corresponding cranial nerve, derived from neuroectoderm, which innervates its muscular derivatives.
- Thus, every pharyngeal arch contains a characteristic combination of cartilage, muscle, artery, and nerve, forming the basis of organized head and neck development.

Skeletal Elements of the Pharyngeal Arches
- Migrating neural crest cells form a cartilaginous core within each pharyngeal arch. The fate of this cartilage varies: certain portions persist, some regress, others undergo endochondral ossification to form bone, and parts of the perichondrium may remain as ligaments. These transformations contribute significantly to the skeletal framework of the head and neck.
First Pharyngeal Arch
- The first pharyngeal arch divides into a smaller cranial maxillary process and a larger caudal mandibular process. Its cartilaginous components develop between days 41 and 45 of embryonic life.
- The cartilage of the maxillary component is termed the palatopterygoquadrate cartilage.
- The cartilage of the mandibular component is known as Meckel’s cartilage.
- From the dorsal portion of the first arch cartilage arise:
- Malleus
- Incus
- The anterior ligament of the malleus and the sphenomandibular ligament develop from the perichondrium of Meckel’s cartilage.
- Importantly, Meckel’s cartilage does not directly form the mandible. Instead, the body of the mandible develops by intramembranous ossification within the surrounding mesenchyme adjacent to Meckel’s cartilage.
- The maxillary process contributes to formation of the premaxilla, maxilla, zygomatic bone, and part of the temporal bone, and also forms structures of the upper lip and palate. The palatopterygoquadrate cartilage contributes to the incus and parts of the sphenoid region.
Second Arch Cartilage
- The cartilage of the second pharyngeal (hyoid) arch is known as Reichert’s cartilage. It develops between days 45 and 48 of embryogenesis and contributes to several important skeletal structures of the head and neck.
- Derivatives of Reichert’s Cartilage
- The stapes (middle ear ossicle) from its dorsal portion
- The styloid process of the temporal bone from the dorsal segment
- The lesser horn (lesser cornu) of the hyoid bone from the ventral part
- The upper portion of the body of the hyoid bone from the ventral segment
- The stylohyoid ligament, derived from the perichondrium of the regressing intermediate cartilage between the styloid process and hyoid bone
- These derivatives are clinically relevant in understanding congenital anomalies and surgical anatomy of the middle ear and hyoid region.
Third Arch Cartilage
- In the third pharyngeal arch, the dorsal segment of the cartilage regresses during development. The ventral portion persists and contributes to components of the hyoid bone, specifically:
- The greater horn (greater cornu)
- The inferior part of the body of the hyoid bone
- These structures provide attachment for muscles involved in swallowing and speech.
Fourth and Sixth Arches
- In both the fourth and sixth pharyngeal arches, the dorsal segments of the cartilage disappear. Their ventral components give rise to most of the laryngeal cartilages, including:
- Thyroid cartilage
- Cricoid cartilage
- Arytenoid cartilage
- Corniculate cartilage
- Cuneiform cartilage
- The epiglottic cartilage does not develop from these arches. It arises from the hypobranchial eminence, a midline swelling derived mainly from the third and fourth arches.
- These derivatives form the structural framework of the larynx, essential for airway protection and phonation.
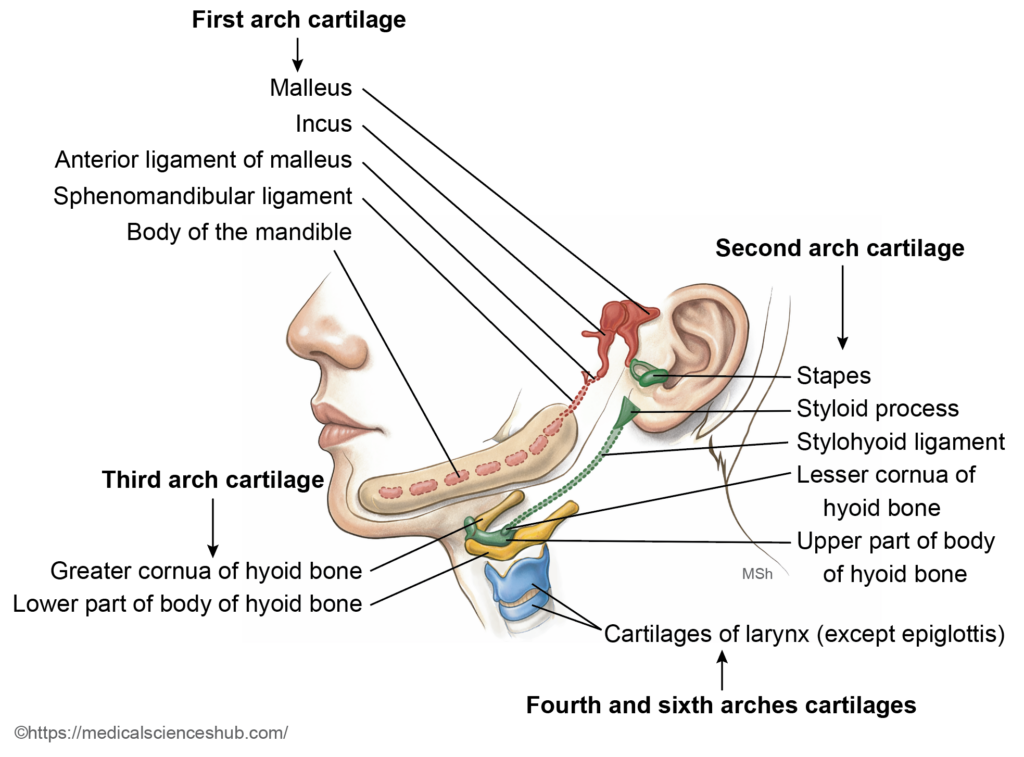
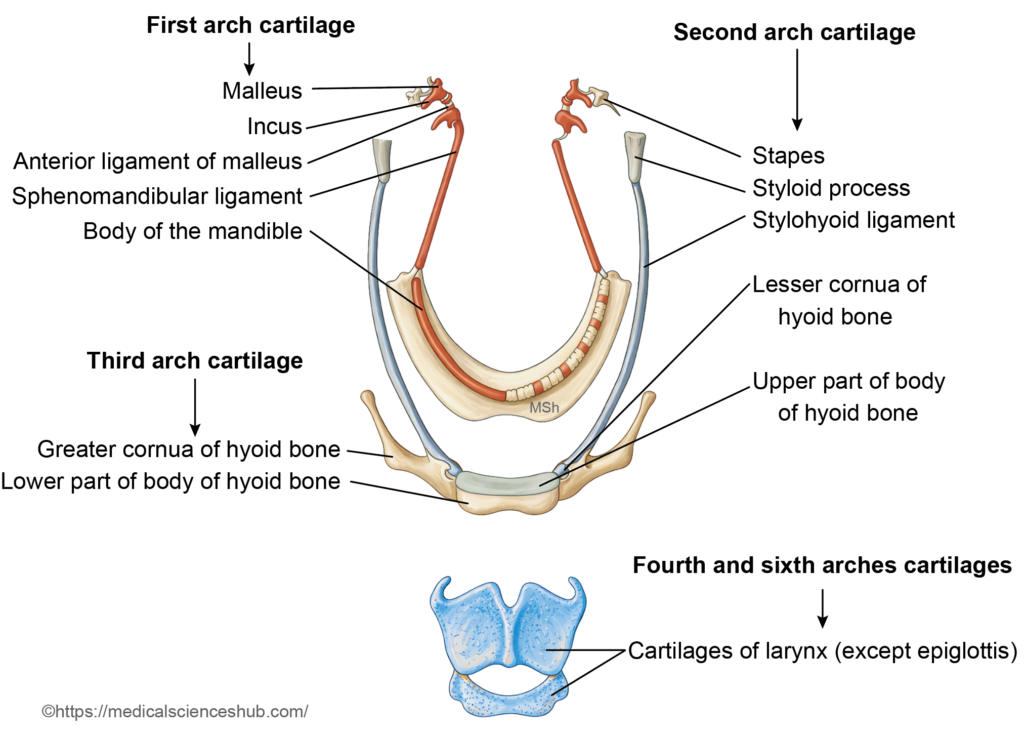
Figure 9.6a: Line diagram: Structures derived from cartilages of the pharyngeal arches (Click to see figure)

Muscular Derivatives of the Pharyngeal Arches
- The mesoderm within each pharyngeal arch differentiates into striated (skeletal) muscle. As these muscles migrate to their final anatomical positions, they retain the nerve supply of their arch of origin. This pattern explains the segmental innervation of head and neck muscles.
First Arch
- Muscles derived from the first arch include:
- The muscles of mastication: temporalis, masseter, medial pterygoid, and lateral pterygoid
- Tensor tympani
- Tensor veli palatini
- Anterior belly of digastric
- Mylohyoid
- Nerve supply: These muscles are innervated by the mandibular division of the trigeminal nerve (cranial nerve V3).
Second Arch
- Muscles derived from the second arch include:
- Muscles of facial expression
- Posterior belly of digastric
- Stapedius
- Stylohyoid
- Nerve supply: These muscles receive innervation from the facial nerve (cranial nerve VII).
Third Arch
- The third pharyngeal arch gives rise to the stylopharyngeus muscle, which elevates the pharynx during swallowing and speech.
- Nerve supply: It is innervated by the glossopharyngeal nerve (cranial nerve IX), the nerve of the third arch.
Fourth Arch
- Muscles derived from the fourth arch include:
- Cricothyroid muscle
- Pharyngeal constrictor muscles
- All palatal muscles except the tensor veli palatini
- Nerve supply: These muscles are supplied by the superior laryngeal branch of the vagus nerve (cranial nerve X).
Sixth Arch
- The sixth arch forms all intrinsic muscles of the larynx, except the cricothyroid muscle.
- Nerve supply: These muscles are innervated by the recurrent laryngeal branch of the vagus nerve.
- Note: The carotid body develops from the third arch region, whereas the aortic bodies are associated with derivatives of the fourth arch. These structures function as peripheral chemoreceptors involved in regulation of respiration.
Table 9.1 : Derivatives of the pharyngeal (branchial) arches
| Arch | Muscles | Nerve (CN) | Skeletal Derivatives and ligaments |
|---|---|---|---|
| 1st (Meckel’s cartilage) | Muscles of mastication Tensor veli palatini Tensor tympani Mylohyoid Anterior belly of digastric | Trigeminal (CN V3) | Maxilla, zygomatic, part of temporal bone; malleus, incus; mandibular development guided by Meckel’s cartilage Anterior ligament of malleus, sphenomandibular ligament |
| 2nd (Reichert’s cartilage) | Muscles of facial expression Stapedius Stylohyoid Posterior belly of digastric | Facial (CN VII) | Stapes Styloid process Lesser horn and upper body of hyoid Stylohyoid ligament |
| 3rd | Stylopharyngeus | Glossopharyngeal (CN IX) | Greater horn and lower body of hyoid |
| 4th | Cricothyroid Levator veli palatini Pharyngeal constrictors | Vagus (CN X, superior laryngeal) | Thyroid cartilage; parts of arytenoid, corniculate, cuneiform |
| 6th | Intrinsic laryngeal muscles (except cricothyroid) | Vagus (CN X, recurrent laryngeal) | Cricoid cartilage; parts of arytenoid, corniculate, cuneiform |
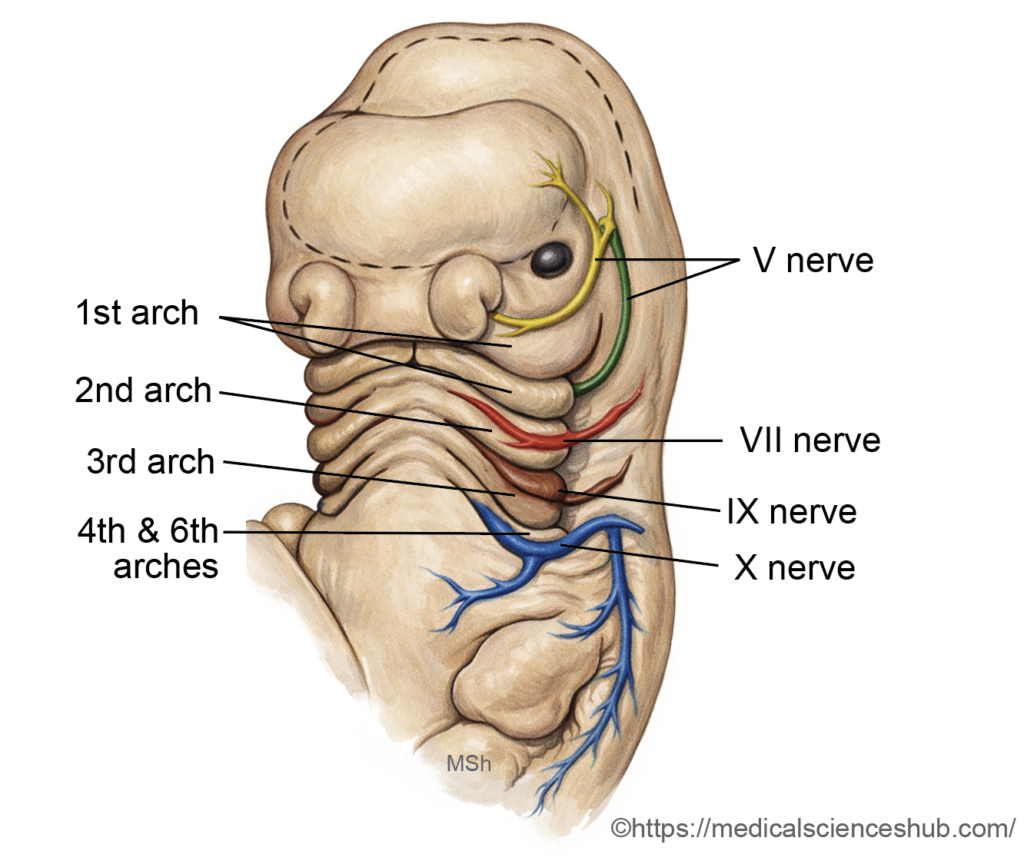
Nerves of Pharyngeal Arches
- Each pharyngeal arch is supplied by a specific cranial nerve that arises from nuclei in the developing hindbrain (rhombencephalon). During early development, the nerve of each arch divides near the corresponding pharyngeal cleft into a pretrematic branch (passing cranial to the cleft) and a post-trematic branch (passing caudal to the cleft).
- In most arches, the pretrematic branch regresses. An exception occurs in the first arch, where the chorda tympani (a branch of the facial nerve, CN VII) represents the persistent pretrematic component. However, it does not supply first-arch muscles; instead, it carries taste fibers from the anterior two-thirds of the tongue and parasympathetic fibers to salivary glands.
- The nerve associated with each arch is a mixed nerve, providing branchiomotor (special visceral efferent) fibers to arch-derived muscles and sensory fibers to derivatives of the pharyngeal pouches, clefts, and related mucosa.
- The cranial nerves of the pharyngeal arches are:
- First arch: The trigeminal nerve (CN V). The mandibular division (V3) supplies the muscles (post-trematic component), while sensory supply is mainly through the maxillary (V2) and mandibular (V3) divisions.
- Second arch: The facial nerve (CN VII).
- Third arch: The glossopharyngeal nerve (CN IX).
- Fourth arch: The superior laryngeal branch of the vagus nerve (CN X).
- Sixth arch: The recurrent laryngeal branch of the vagus nerve (CN X).
- The fifth arch is rudimentary in humans and does not give rise to definitive adult structures.
Somites and Somitomeres in Pharyngeal Arches
- Musculature of the pharyngeal arches develops from paraxial mesoderm, which is organized into somitomeres (1–7) in the cranial region and occipital somites (1–5) caudally. These mesodermal segments migrate into specific arches and differentiate into their characteristic skeletal muscles.
- Somitomeres primarily contribute to muscles of the first and second arches, whereas occipital somites are largely responsible for muscles derived from the third, fourth, and sixth arches. This segmental origin explains the distinct and consistent pattern of cranial nerve innervation of each arch.
Table 9.2: Contribution of somitomeres and occipital somites to cranial musculature
| Segment | Muscles Derived | Nerve Supply |
|---|---|---|
| Somitomeres 1–2 | Extraocular muscles (SR, IR, MR, IO, levator palpebrae superioris) | Oculomotor nerve |
| Somitomere 3 | Superior oblique | Trochlear nerve |
| Somitomere 4 | 1st arch muscles: mastication, mylohyoid, anterior digastric, tensor veli palatini, tensor tympani | Trigeminal nerve |
| Somitomere 5 | Lateral rectus | Abducens nerve |
| Somitomere 6 | 2nd arch muscles: facial expression, stapedius, stylohyoid, posterior digastric | Facial nerve |
| Somitomere 7 | Stylopharyngeus (3rd arch) | Glossopharyngeal nerve |
| Occipital somites 1–2 | 4th arch muscles: cricothyroid, pharyngeal constrictors | Vagus nerve (superior laryngeal branch) |
| Occipital somites 3–4 | Tongue muscles (except palatoglossus) | Hypoglossal nerve |
Arteries of the Pharyngeal Arches (Aortic Arches)
- Each pharyngeal arch is associated with a paired aortic arch artery. These vessels arise from the aortic sac anteriorly and connect to the paired dorsal aortae posteriorly. During embryonic development, the aortic arches undergo selective regression and remodeling to form major arteries of the head, neck, and thorax.
- The derivatives of the aortic arches are as follows:
- First Aortic Arch
Most of this arch regresses. A small remnant persists as part of the maxillary artery, a branch of the external carotid artery. - Second Aortic Arch
Largely disappears during development. Its remnants form the stapedial artery and the hyoid artery, which are transient vessels in humans and usually regress before birth. - Third Aortic Arch
Plays a major role in carotid circulation.- The ventral portion forms the common carotid artery.
- The dorsal portion contributes to the proximal part of the internal carotid artery.
(The distal internal carotid artery develops from the cranial segment of the dorsal aorta.)
- Fourth Aortic Arch
Shows asymmetrical development:- On the right side, it forms the proximal segment of the right subclavian artery.
- On the left side, it becomes part of the arch of the aorta between the left common carotid and left subclavian arteries.
- Fifth Aortic Arch
This arch is either rudimentary or never fully develops in humans and leaves no definitive adult derivative. - Sixth Aortic Arch (Pulmonary Arch)
Contributes to the pulmonary circulation:- On the right side, it forms the proximal part of the right pulmonary artery.
- On the left side, it forms the proximal left pulmonary artery and the ductus arteriosus, which after birth becomes the ligamentum arteriosum.
- First Aortic Arch
- This transformation of the aortic arches establishes the definitive arterial pattern of the great vessels in the adult cardiovascular system.
CLINICAL EMBRYOLOGY
First arch syndromes
- It results from defective migration or differentiation of neural crest cells into the first pharyngeal (mandibular) arch. Neural crest cells form most of the skeletal elements and connective tissue of this arch. Impaired development therefore primarily affects the mandible, zygomatic region, and external ear. The two principal conditions are Treacher Collins syndrome and Pierre Robin sequence.
- Treacher Collins Syndrome (Mandibulofacial Dysostosis)
- Treacher Collins syndrome is an autosomal dominant disorder caused most commonly by mutations in the TCOF1 gene on chromosome 5. The gene product, treacle, is required for normal proliferation and survival of neural crest cells during craniofacial development. The condition occurs in approximately 1 in 50,000 live births.
- Clinical features include:
- Mandibular hypoplasia, producing a small and retruded lower jaw
- Malar (zygomatic) hypoplasia, leading to flattened cheeks
- Downward-slanting palpebral fissures
- External ear anomalies, such as malformed pinna and external auditory canal atresia, which may cause conductive hearing loss
- The severity varies widely, even within affected families.
- Pierre Robin Sequence
- It is characterized by a triad of:
- Micrognathia (small mandible)
- Glossoptosis (posterior displacement of the tongue)
- Cleft palate
- The mandibular hypoplasia leads to posterior displacement of the tongue, which interferes with palatal fusion; hence, it is termed a sequence rather than a primary syndrome. The incidence is approximately 1 in 10,000–15,000 births.
- Pierre Robin sequence may occur in isolation or as part of broader genetic conditions. It has been associated with abnormalities involving chromosomes 2, 11, and 17, including mutations affecting the SOX9 gene, which plays a critical role in craniofacial cartilage development.
- Both conditions illustrate the essential role of neural crest cell migration and differentiation in first arch development and normal craniofacial formation.
- It is characterized by a triad of:
PHARYNGEAL CLEFTS
Definition
- Pharyngeal clefts are surface depressions formed by ectoderm between adjacent pharyngeal arches during early embryonic development. In humans, four clefts are present externally.
- Only the dorsal part of the first pharyngeal cleft persists in the adult. It develops into the epithelial lining of the external acoustic meatus and contributes to the outer (ectodermal) layer of the tympanic membrane. The remaining clefts normally regress and do not form definitive adult structures.
Cervical Sinus
- During development, the second pharyngeal arch enlarges rapidly and extends caudally, overlapping the third and fourth arches. As a result, the second, third, and fourth clefts become enclosed beneath this overgrowth. The buried clefts form a temporary ectoderm-lined cavity known as the cervical sinus.
- The cervical sinus is transient and normally disappears as the neck develops, producing a smooth external contour without visible grooves. Failure of complete obliteration may result in branchial cysts, sinuses, or fistulae, which are congenital anomalies along the lateral aspect of the neck.
CLINICAL EMBRYOLOGY
Branchial (Cervical) Cyst
- A branchial cyst is a congenital epithelial cyst that appears along the lateral aspect of the neck. It most commonly arises from incomplete obliteration of the second pharyngeal cleft and the associated cervical sinus.
- Location:It is typically situated along the anterior border of the sternocleidomastoid muscle, often near the angle of the mandible.
- Cause: During normal development, the second pharyngeal arch overgrows the third and fourth arches, burying the second to fourth clefts. If this overgrowth or subsequent obliteration fails, remnants of the cleft epithelium persist and form a cystic cavity.
- Clinical features:
- Presents as a smooth, painless swelling on the lateral side of the neck.
- It is usually not evident at birth but becomes noticeable later in childhood or early adulthood.
- The swelling may enlarge during upper respiratory tract infections due to secondary inflammation.
- Pathology:The cyst wall is lined by either:
- Stratified squamous epithelium, or
- Ciliated columnar epithelium, reflecting its pharyngeal origin.
- Treatment:Definitive management is complete surgical excision. Incomplete removal of the epithelial tract may result in recurrenc.
Branchial Fistula and Sinus
Persistent communication between the cyst and surrounding structures produces different anomalies:
- A complete branchial fistula has openings both on the skin of the neck and internally into the pharynx.
- An internal branchial sinus communicates only with the pharyngeal lumen.
- An external branchial sinus opens only onto the skin surface.
These anomalies also arise most commonly from persistence of the second pharyngeal cleft and its tract.
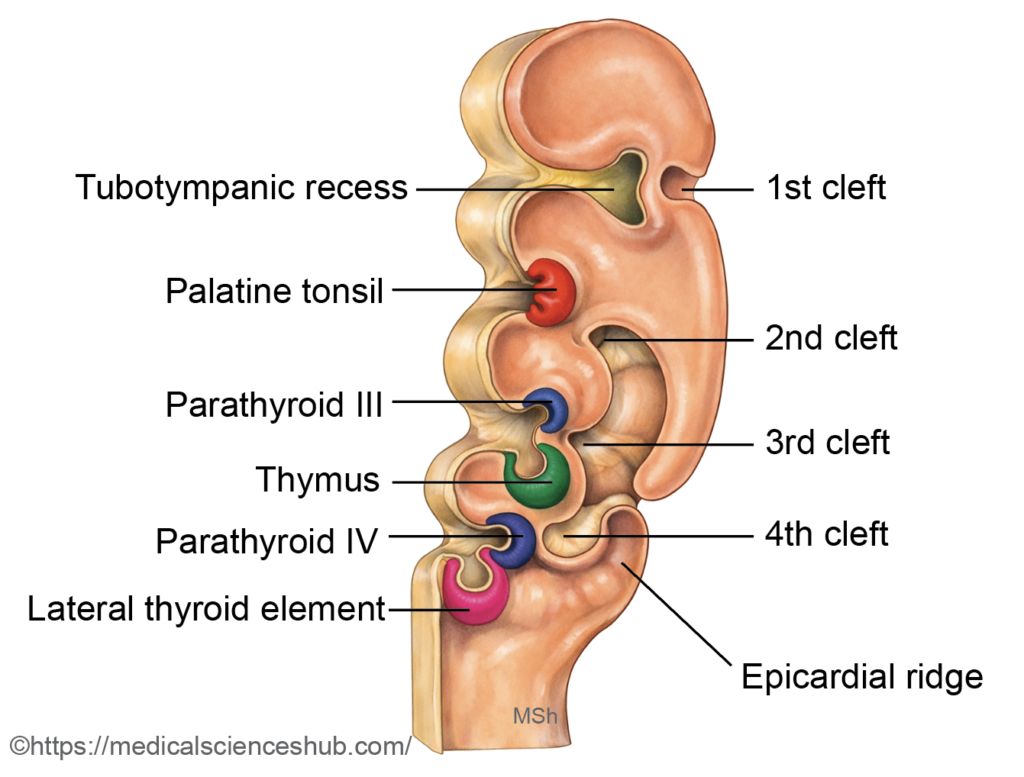
PHARYNGEAL POUCHES
- Pharyngeal pouches are endoderm-lined outpocketings that arise from the lateral wall of the primitive pharynx. In humans, five pairs develop in a cranio-caudal sequence. The fifth pouch is rudimentary and is commonly regarded as part of the fourth pouch complex.
- The right and left pouches approach each other ventrally and contribute to the formation of the floor of the primitive pharynx. This region later participates in the development of the tongue and adjacent pharyngeal structures.
- Each pouch gives rise to specific epithelial derivatives in the head and neck, including components of the middle ear, tonsillar tissue, and several endocrine glands. Their principal derivatives are summarized in standard embryologic classifications.
First Pouch
- The first pharyngeal pouch is an endodermal outgrowth from the primitive pharynx. Its ventral portion becomes compressed and largely disappears as the tongue develops.
- The dorsal portion expands laterally to form the tubotympanic recess.
- The proximal part of this recess develops into the pharyngotympanic (Eustachian) tube.
- The distal part forms the tympanic (middle ear) cavity and contributes to the mastoid antrum and mastoid air cells.
- The endoderm of the first pouch also gives rise to the inner epithelial lining of the tympanic membrane. (The outer epithelial layer is derived from the first pharyngeal cleft.)
Second Pouch
- The second pharyngeal pouch develops caudal to the first pouch and differentiates into dorsal and ventral components.
- The ventral part forms the epithelial lining of the palatine tonsil and the tonsillar crypts. The lymphoid tissue of the tonsil arises later from surrounding mesenchyme (mesoderm), not from endoderm.
- A persistent deep recess within the tonsil, known as the intratonsillar cleft (crypta magna), represents a remnant of the second pouch cavity.
Third Pouch
- The third pharyngeal pouch differentiates into distinct dorsal and ventral wings, each forming important endocrine structures.
- The dorsal wing develops into the inferior parathyroid glands (parathyroid III).
- The ventral wing gives rise to the thymus.
- During development, both wings detach from the pharyngeal wall and migrate caudally. The thymic primordia descend into the superior part of the anterior mediastinum, where the thymus attains its definitive position. The inferior parathyroid glands initially migrate together with the thymus but later separate and attach to the lower poles of the thyroid gland. Their longer descent explains their variable final position.
- The epithelial framework of the thymus is derived from endoderm of the third pouch, including the formation of Hassall’s corpuscles. In contrast, thymocytes originate from hematopoietic stem cells in the bone marrow (mesodermal origin) and subsequently migrate into the developing thymus for maturation.
Fourth Pouch
- The fourth pharyngeal pouch develops a dorsal and a ventral component.
- The dorsal wing forms the superior parathyroid glands (parathyroid IV). After separating from the pharyngeal wall, these primordia migrate caudally and eventually attach to the posterior aspect of the lateral lobes of the thyroid gland. Although termed “superior,” their final position is higher than the inferior parathyroids because they undergo a shorter migratory descent.
- The ventral part of the fourth pouch contributes to the ultimobranchial body, which later becomes incorporated into the thyroid gland and gives rise to parafollicular (C) cells that secrete calcitonin.
Fifth Pouch
- In humans, the fifth pharyngeal pouch is rudimentary and transient. It is generally considered part of the fourth pouch complex. When identifiable, it contributes to the formation of the ultimobranchial body, which integrates into the thyroid gland during development.
Caudal pharyngeal complex
- The caudal pharyngeal complex is formed by the fusion of the ventral part of the fourth pharyngeal pouch with the rudimentary fifth pouch. This combined structure contributes to several important components of the developing neck.
- It differentiates into the following elements:
- Thymic component:
A small portion may become incorporated into the developing thymus, supplementing the major thymic tissue derived from the third pouch. - Lateral thyroid component:
This portion merges with the median thyroid primordium, which originates from the thyroglossal duct. Fusion of these elements contributes to definitive thyroid formation and stabilizes its final position in the neck. - Ultimobranchial body:
This structure becomes integrated into the thyroid gland and gives rise to the parafollicular (C) cells, which secrete calcitonin.
- Thymic component:
- The neural crest cells migrate into the ultimobranchial body and differentiate into parafollicular cells. Thus, although the ultimobranchial body is endodermal in origin, its functional endocrine cells are derived from neural crest.
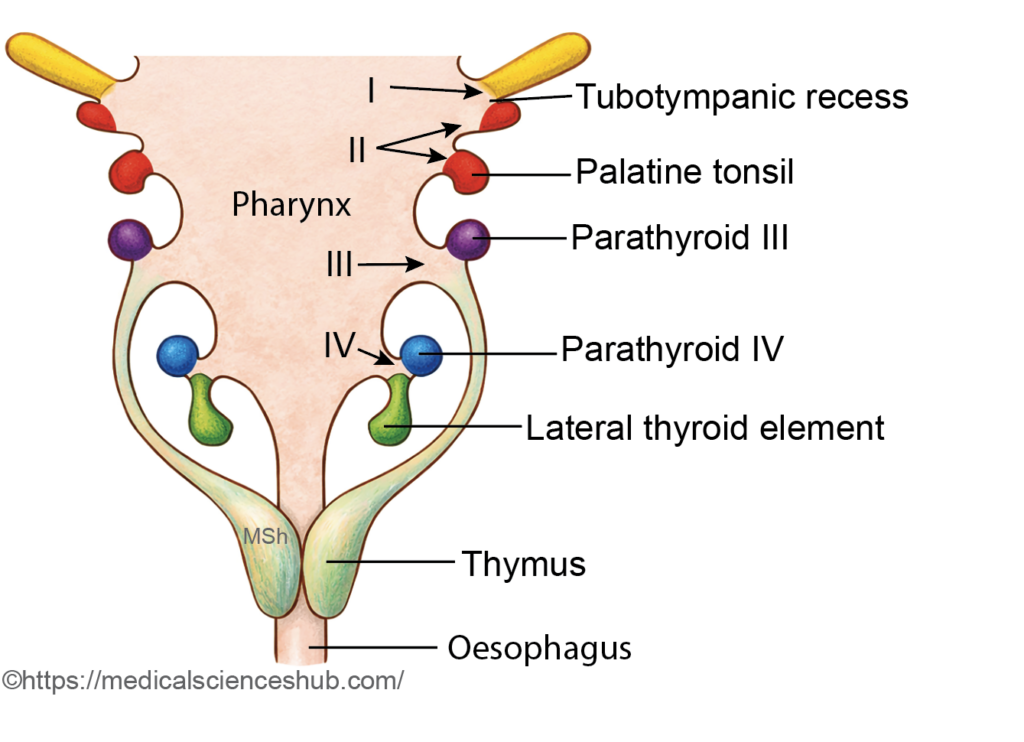
Table 9.3: Derivatives of pharyngeal pouches
| Pouch | Adult Derivatives | Key Points |
|---|---|---|
| 1st | Pharyngotympanic tube Middle ear cavity Inner layer of tympanic membrane | Forms tubotympanic recess; outer membrane layer from 1st cleft |
| 2nd | Epithelium of palatine tonsil and tonsillar fossa | Lymphoid tissue from mesenchyme; epithelium is endodermal |
| 3rd | Dorsal: inferior parathyroids; Ventral: thymus | Both detach and descend; parathyroids migrate with thymus |
| 4th | Dorsal: superior parathyroids | Migrates and attaches to upper posterior thyroid |
| Caudal pharyngeal complex (Ventral 4th pouch + rudimentary 5th pouch) | Ultimobranchial body → parafollicular (C) cells Minor thymic/thyroid components | Endodermal origin C cells derived from neural crest |
Development of Palatine Tonsil
- The palatine tonsil has a dual origin. Its epithelial component is derived from the endoderm of the second pharyngeal pouch, while its lymphoid tissue develops from mesenchymal cells (mesoderm) that later differentiate into lymphocytes.
Stages of Development
- During the third month of intrauterine life, the ventral part of the second pharyngeal pouch proliferates into the surrounding mesenchyme as multiple solid epithelial projections known as tonsillar buds.
- Subsequently, the central cells of these buds undergo degeneration, resulting in the formation of hollow spaces called tonsillar crypts. Between the third and fifth months, lymphocytes accumulate in the adjacent mesenchyme and organize into lymphoid follicles around the crypts. Progressive lymphocytic proliferation produces the characteristic tonsillar prominence in the lateral wall of the oropharynx.
- The surrounding mesenchyme condenses to form a partial fibrous capsule on the lateral aspect of the tonsil.
- A persistent remnant of the second pouch cavity may remain as the intratonsillar cleft, and the surface depression in which the tonsil lies is termed the tonsillar fossa.
Development of Thymus
- The thymus originates from two principal sources:
- The endoderm of the third pharyngeal pouch, which forms the epithelial framework.
- Surrounding mesenchyme (mesoderm), which contributes connective tissue components.
- Importantly, thymocytes are not mesodermal derivatives of the pouch itself; they arise from hematopoietic stem cells in the bone marrow and later migrate into the developing thymus.
Stages of Development
- By the end of the fourth week, paired thymic primordia appear as endodermal proliferations from the ventral part of the third pharyngeal pouches. These initially form hollow epithelial outgrowths that extend into adjacent mesenchyme and subsequently transform into solid, branching epithelial cords. These cords organize into the structural basis of future thymic lobules.
- Between the fourth and seventh weeks, the thymic primordia detach from the pharyngeal wall and migrate caudally and medially. They descend to a position inferior and anterior to the thyroid gland, ultimately lying in the anterior mediastinum, posterior to the sternum. The right and left components fuse to form a bilobed gland.
- The thymus is initially epithelial in nature. It becomes infiltrated by mesenchymal cells, which form the capsule and internal septa. By the third month, lymphocytes derived from the bone marrow populate the gland. Around the twelfth week, the thymic lobules differentiate into a peripheral cortex and a central medulla. Within the medulla, epithelial cells organize into Hassall’s corpuscles, structures involved in immune regulation. The thymic epithelial reticulum is derived from endoderm.
Postnatal Changes
- The thymus enlarges from birth until puberty. After puberty, it gradually decreases in size through a process known as thymic involution, in which functional tissue is progressively replaced by adipose tissue.
Development of Parathyroid Gland
Humans typically have four parathyroid glands, arranged as two superior and two inferior glands. Their development is closely related to the third and fourth pharyngeal pouches.
- The inferior parathyroid glands arise from the dorsal wing of the third pharyngeal pouch.
- The superior parathyroid glands develop from the dorsal wing of the fourth pharyngeal pouch.
Stages of Development
- The dorsal part of the third pharyngeal pouch proliferates, detaches from the pharyngeal wall, and migrates caudally together with the developing thymus (derived from the ventral wing of the same pouch). During descent, the parathyroid tissue separates from the thymus and ultimately attaches to the posterior surface of the lower poles of the thyroid gland, forming the inferior parathyroid glands.
- The dorsal part of the fourth pharyngeal pouch also detaches from the pharynx and migrates a shorter distance. It comes to rest on the posterior aspect of the upper poles of the thyroid gland, forming the superior parathyroid glands.
- Although termed “inferior” and “superior,” the naming reflects their final anatomical position rather than their pouch of origin. The longer migratory pathway of the third pouch explains the greater variability in the location of the inferior parathyroid glands.
Development of Thyroid Gland
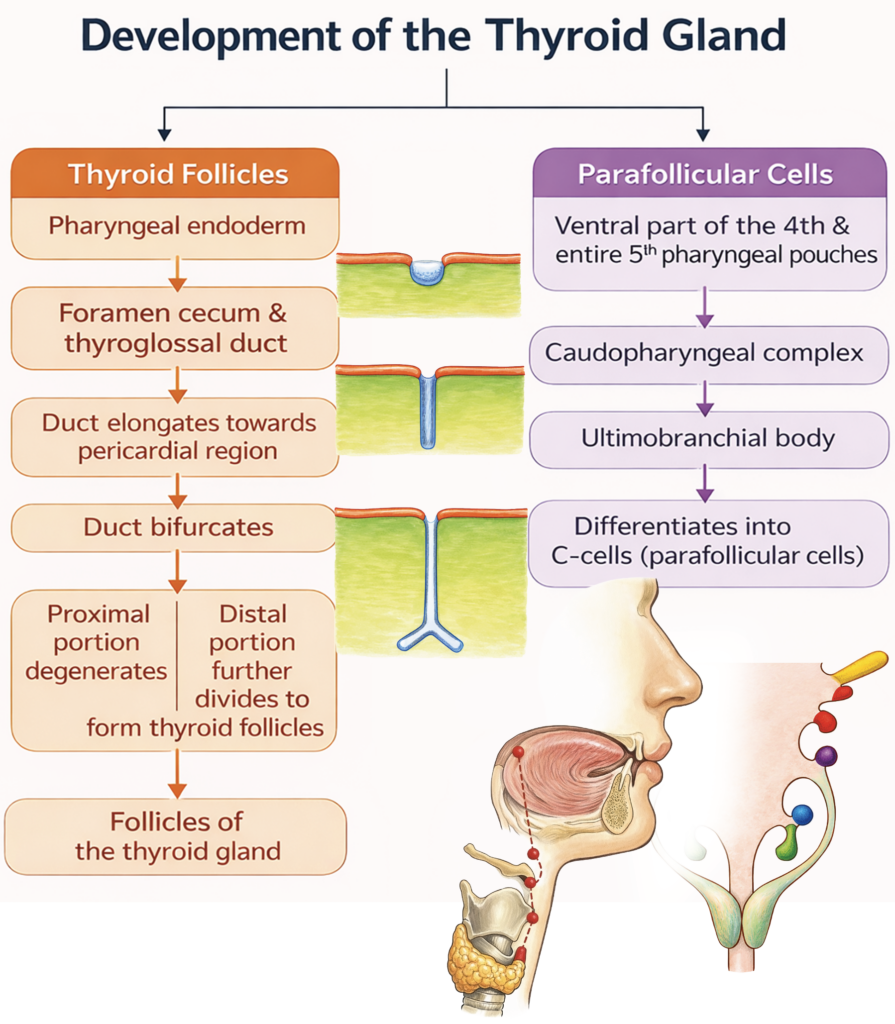
The thyroid gland develops from two embryological sources:
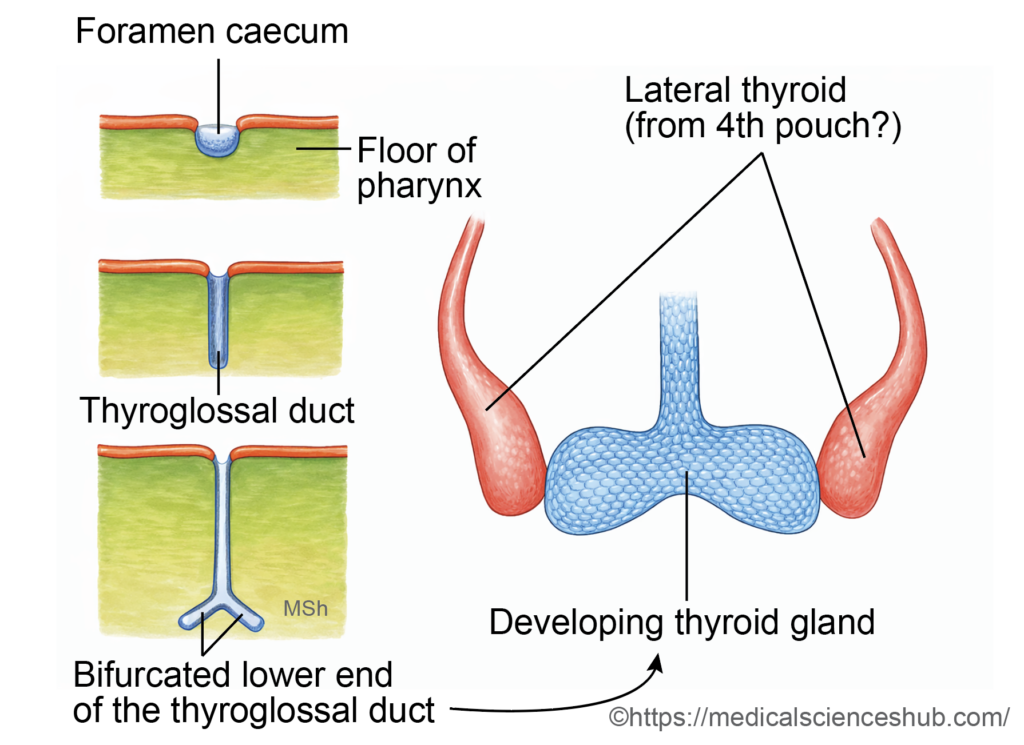
- Follicular cells arise from a midline endodermal thickening that forms the thyroglossal duct.
- Parafollicular (C) cells originate from the ultimobranchial body, which is derived mainly from the fourth (and rudimentary fifth) pharyngeal pouch complex.
The thyroid is the first endocrine gland to begin development in the embryo. By the end of the first trimester (around the 10th–12th week), the follicular cells begin producing thyroid hormones.
Stages of Development
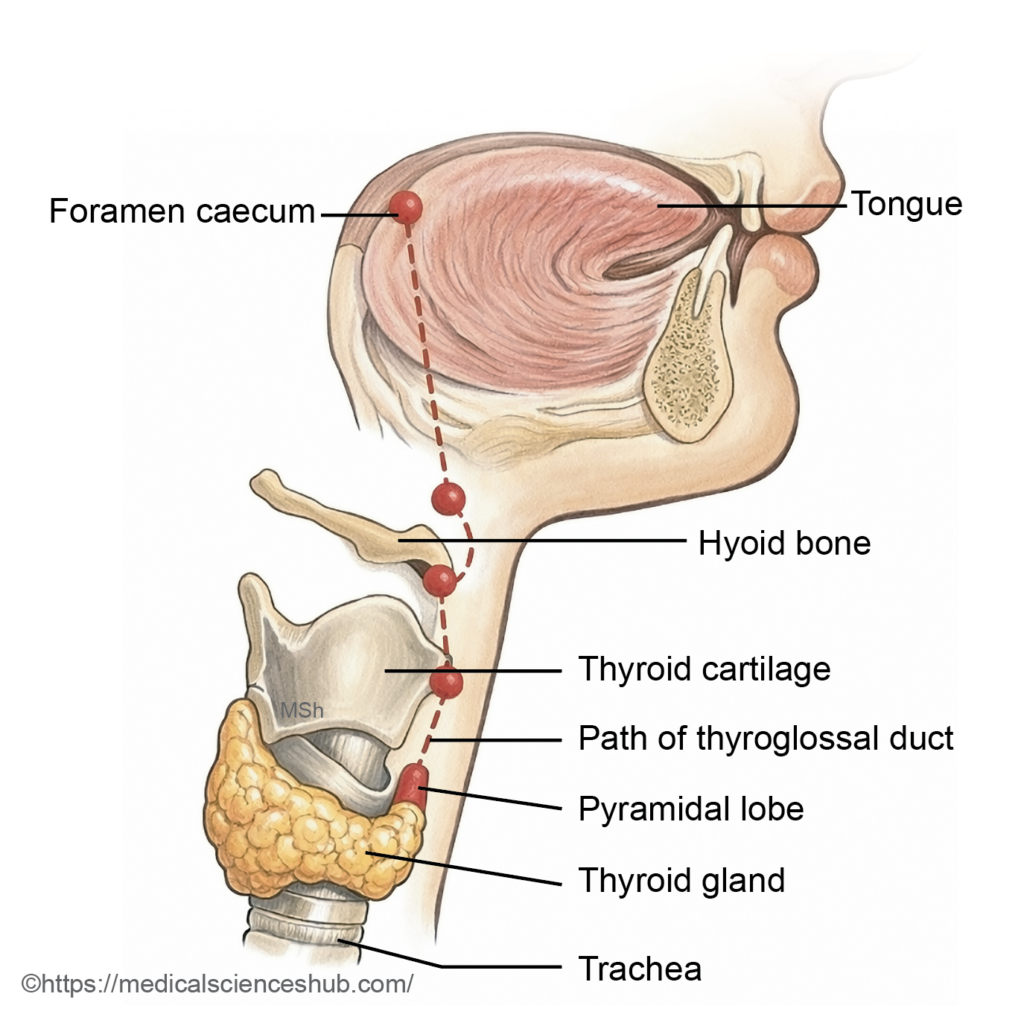
- In the floor of the primitive pharynx, a midline swelling called the tuberculum impar appears between the first and second pharyngeal arches.
- Around the 24th day of development, an endodermal thickening just posterior to this region forms a median diverticulum known as the thyroid primordium. Its opening in the tongue persists as the foramen cecum.
- The primordium elongates inferiorly as the thyroglossal duct, descending in the midline anterior to the developing hyoid bone and laryngeal cartilages.
- By the seventh week, the distal end enlarges and divides to form the right and left lobes of the thyroid gland. The thyroglossal duct normally degenerates thereafter.
- The ultimobranchial bodies later fuse with the developing thyroid and contribute parafollicular (C) cells, which secrete calcitonin.
This coordinated migration and differentiation establish the final position and cellular composition of the thyroid gland in the anterior neck.
CLINICAL EMBRYOLOGY
Anomalies of the Thyroid Gland
- Pyramidal Lobe: A pyramidal lobe is an accessory projection of thyroid tissue that may arise from the isthmus or from either lateral lobe. Its size and length are variable. It represents a persistent remnant of the thyroglossal duct.
- Congenital Hypothyroidism: Congenital hypothyroidism may result from:
- Athyreosis (complete absence of the thyroid gland),
- Thyroid ectopia (abnormal location),
- Thyroid hypoplasia (underdevelopment), or
- Dyshormonogenesis, caused by genetic defects affecting thyroid hormone synthesis.
- Early detection is essential to prevent impaired physical growth and neurodevelopment.
- Thyroid Ectopia: It refers to abnormal positioning of the gland along the developmental pathway of the thyroglossal duct. The most common site is a lingual thyroid at the base of the tongue.
- Ectopic Thyroid Tissue: Ectopic thyroid tissue may also occur outside the normal migratory pathway. Reported sites include the larynx, trachea, esophagus, mediastinum, and, rarely, the ovary (as part of a teratoma, e.g., struma ovarii).
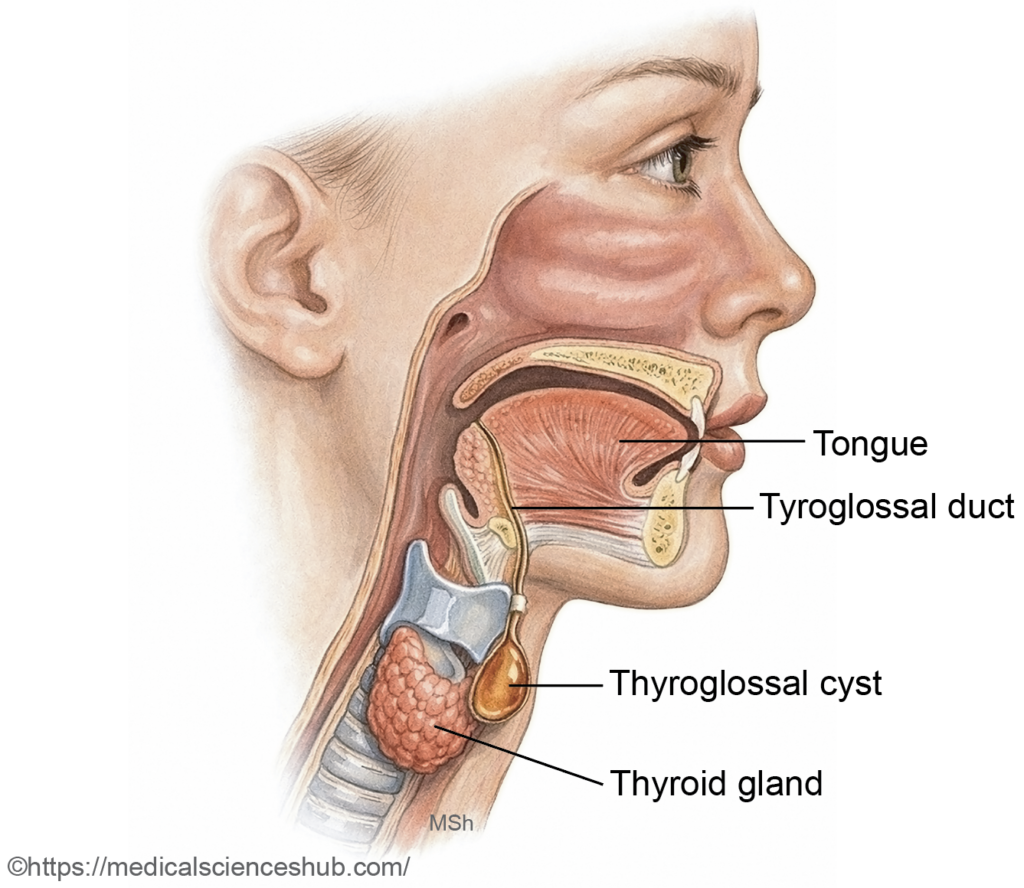
- Thyroglossal cyst and fistula
- The thyroid gland develops from a midline endodermal diverticulum that descends as the thyroglossal duct, which normally undergoes degeneration. Persistence of any ductal segment may lead to a thyroglossal cyst, typically presenting as a painless, midline neck swelling that moves with swallowing and tongue protrusion.
- If the cyst becomes infected or ruptures externally, a persistent tract may form a thyroglossal fistula. Rarely, malignant transformation may occur within a thyroglossal cyst.
Important Questions
- List the derivatives of each pharyngeal pouch.
- List the skeletal derivatives of each pharyngeal arch.
- List the muscular derivatives of each pharyngeal arch and also mention their nerve supply
- Write a short note on first arch syndrome.
- Write a short note on caudopharyngeal complex.
- Write a short note on development of thyroid gland.
- Write a short note on branchial cyst.
- Write a short note on cervical sinus.
