Competencies
- AN79.4: Describe the development of somites and intra-embryonic coelom.
- AN25.2: Describe development of pleura, lung and heart. (Development of pleura is included in this chapter).
- AN52.5: Describe the development and congenital anomalies of diaphragm.
INTRODUCTION
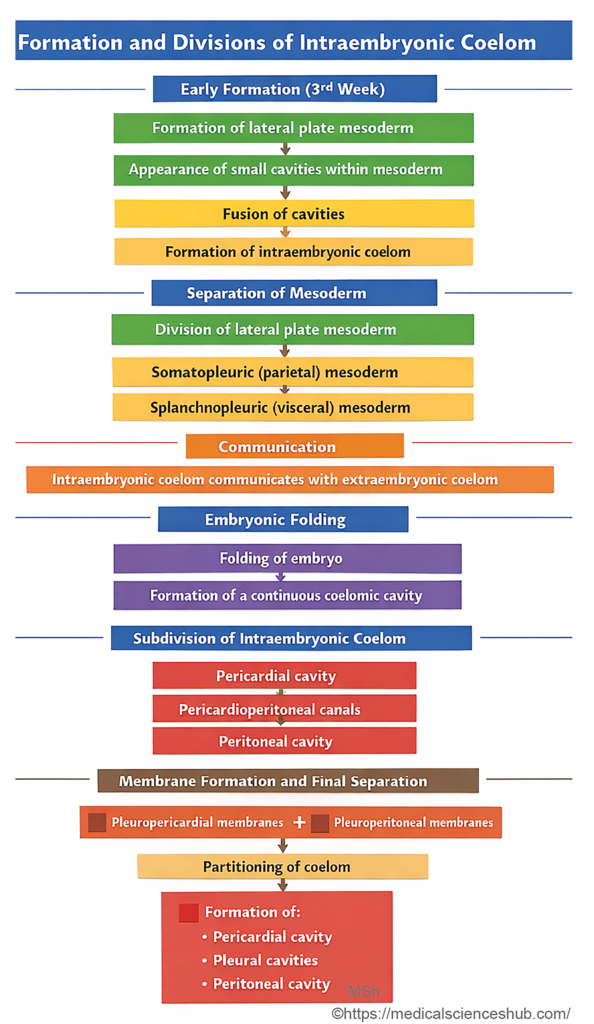
- During the third week of development, small intercellular spaces appear within the lateral plate mesoderm and the pericardial bar. These spaces gradually merge to form a U-shaped primitive intraembryonic coelom.
- The central portion of this cavity develops into the pericardial cavity, while its lateral extensions form the coelomic ducts. These ducts temporarily communicate with the extraembryonic coelom, facilitating the exchange of nutrients during early development.
- The pericardial, pleural, and peritoneal cavities (collectively known as serous cavities) are all derived from the intraembryonic coelom. As this cavity forms, it divides the intraembryonic mesoderm into two layers: the somatopleuric (parietal) layer and the splanchnopleuric (visceral) layer.
- The somatopleuric layer lies adjacent to the ectoderm and laterally becomes continuous with the somatopleuric extraembryonic mesoderm.
- The splanchnopleuric mesoderm lies in contact with the endoderm and laterally continues with the extraembryonic splanchnopleuric mesoderm.
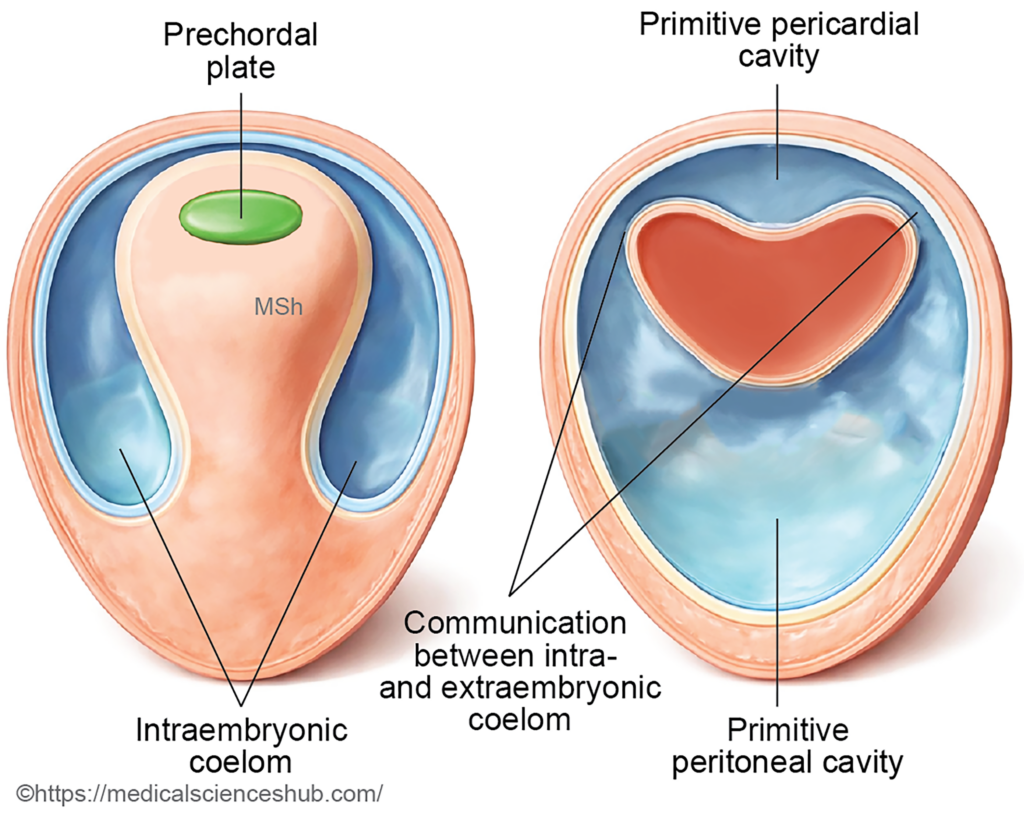
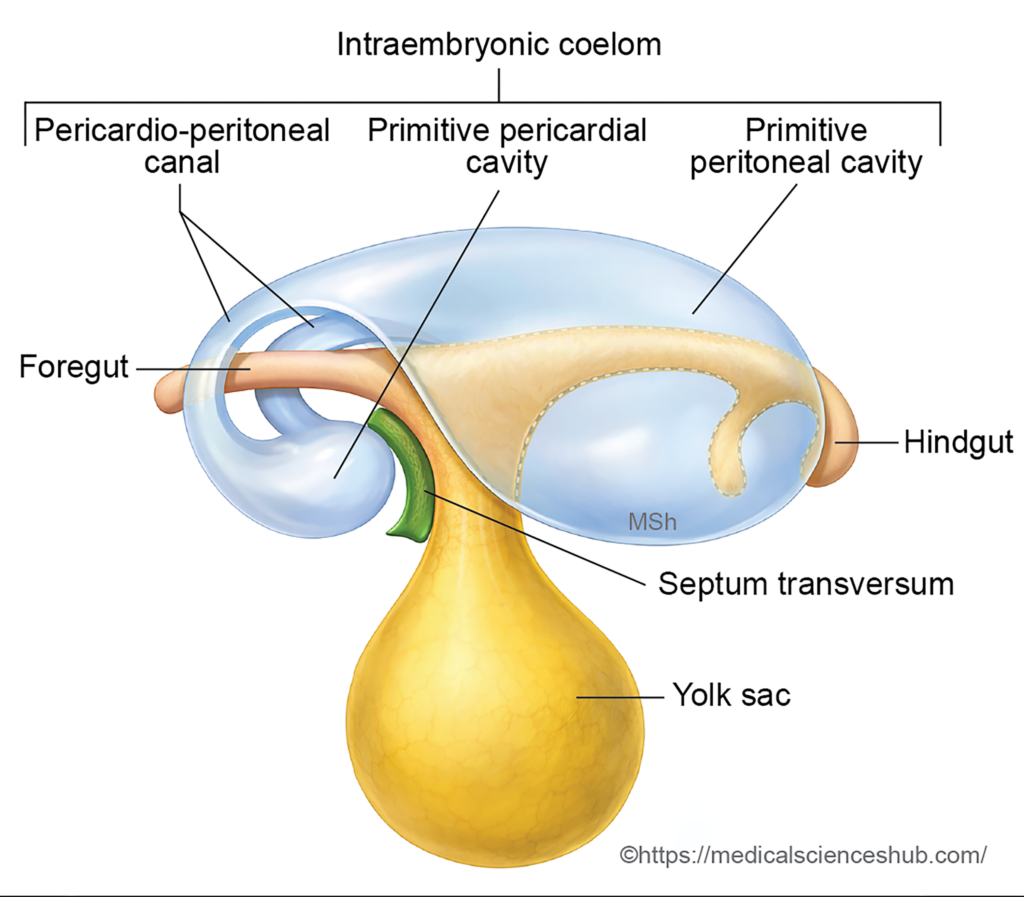
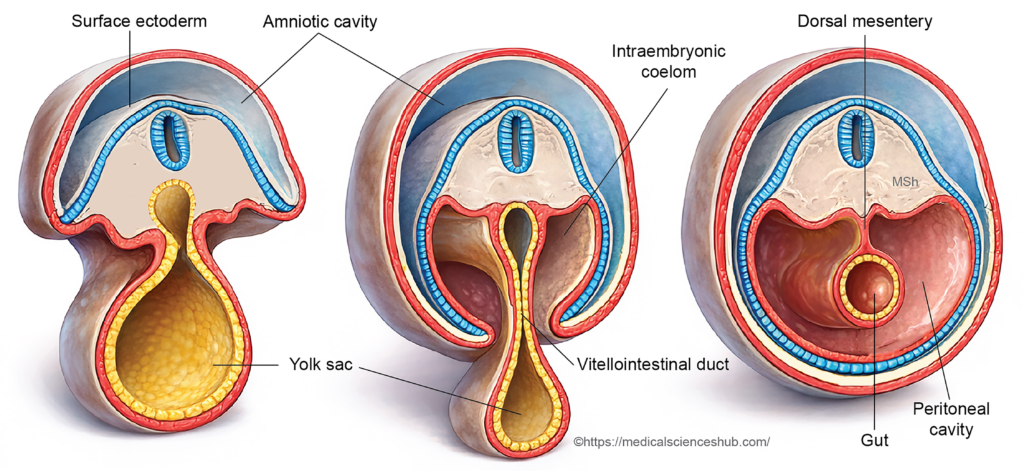
Figure 16.2: Relationship of intraembryonic coelom and gut tube.
Changes Due to Formation of Embryonic Folds
- The formation of embryonic folds alters the spatial arrangement of the intraembryonic coelom. With the development of the head fold, the pericardial cavity shifts to a position ventral to the foregut. It becomes located between the stomodeum anteriorly and the septum transversum posteriorly.
- During the formation of the lateral folds, the ventral portions of the coelomic ducts approach each other and fuse, giving rise to the peritoneal cavity.
- The segments of the coelomic ducts that connect the pericardial cavity with the peritoneal cavity are termed pericardioperitoneal canals. These canals are situated on either side of the developing foregut.
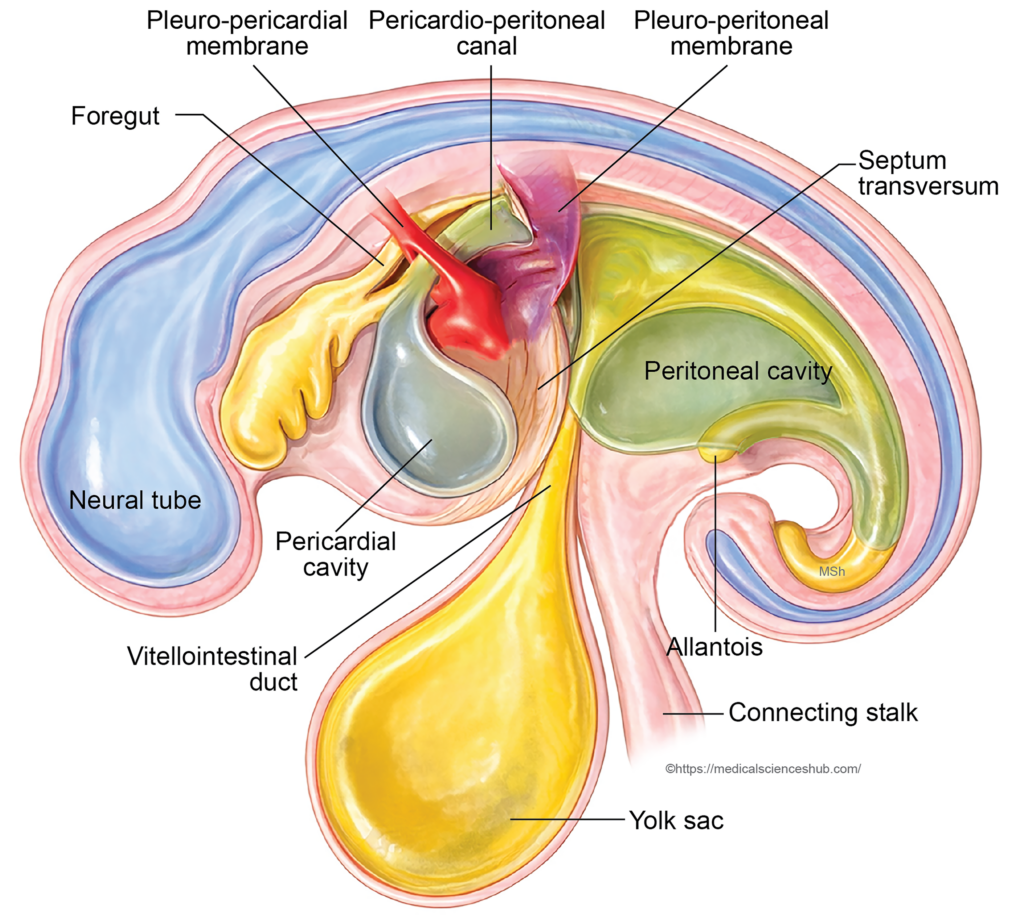
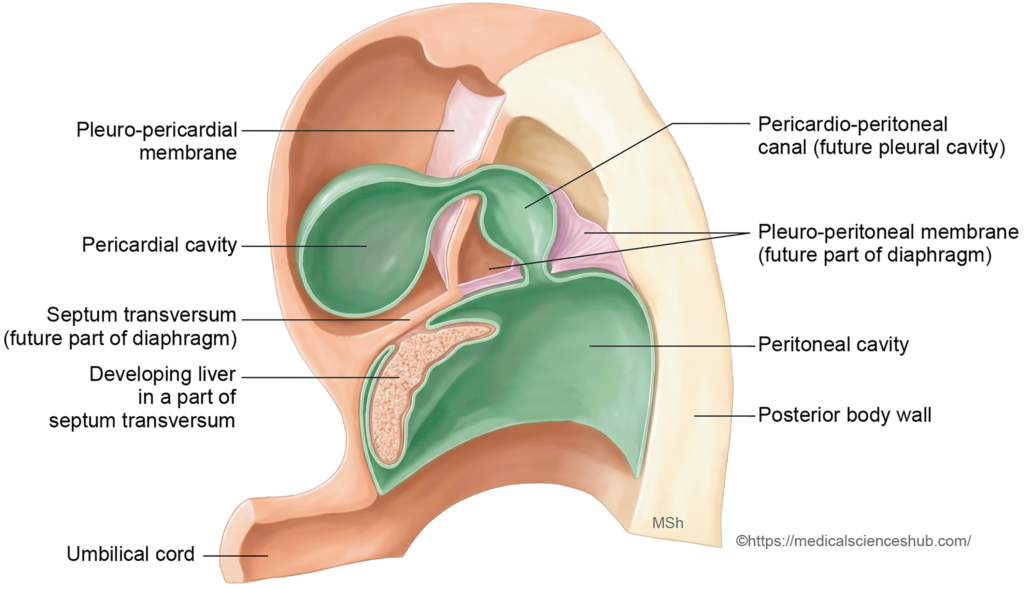
- As the lung buds grow from the foregut, they extend into the pericardioperitoneal canals. Their progressive expansion transforms these canals into the pleural cavities. Subsequently, the pleuropericardial membranes, pleuroperitoneal membranes, and the diaphragm partition the original coelomic space into three separate cavities: the pericardial, pleural, and peritoneal cavities.
Development of the Pericardial Cavity
- The pericardial cavity originates from the midline portion of the intraembryonic coelom located within the pericardial bar. Its position and structural relationships change as embryonic folding progresses.
Stages of Development
- Before formation of the head fold
At this stage, the pericardial cavity lies between the septum transversum anteriorly and the prechordal plate posteriorly. - After formation of the head fold
With cranial folding of the embryo, the pericardial cavity shifts ventrally and comes to lie between the stomodeum anteriorly and the septum transversum posteriorly. Its dorsal relations include the cardiogenic region and the developing foregut. - Formation of the pericardial layers
- The fibrous pericardium and the parietal layer of the serous pericardium arise from the somatopleuric layer of intraembryonic mesoderm.
- The visceral layer of the serous pericardium (epicardium) develops from the splanchnopleuric layer of intraembryonic mesoderm.
DEVELOPMENT OF PLEURAL CAVITY
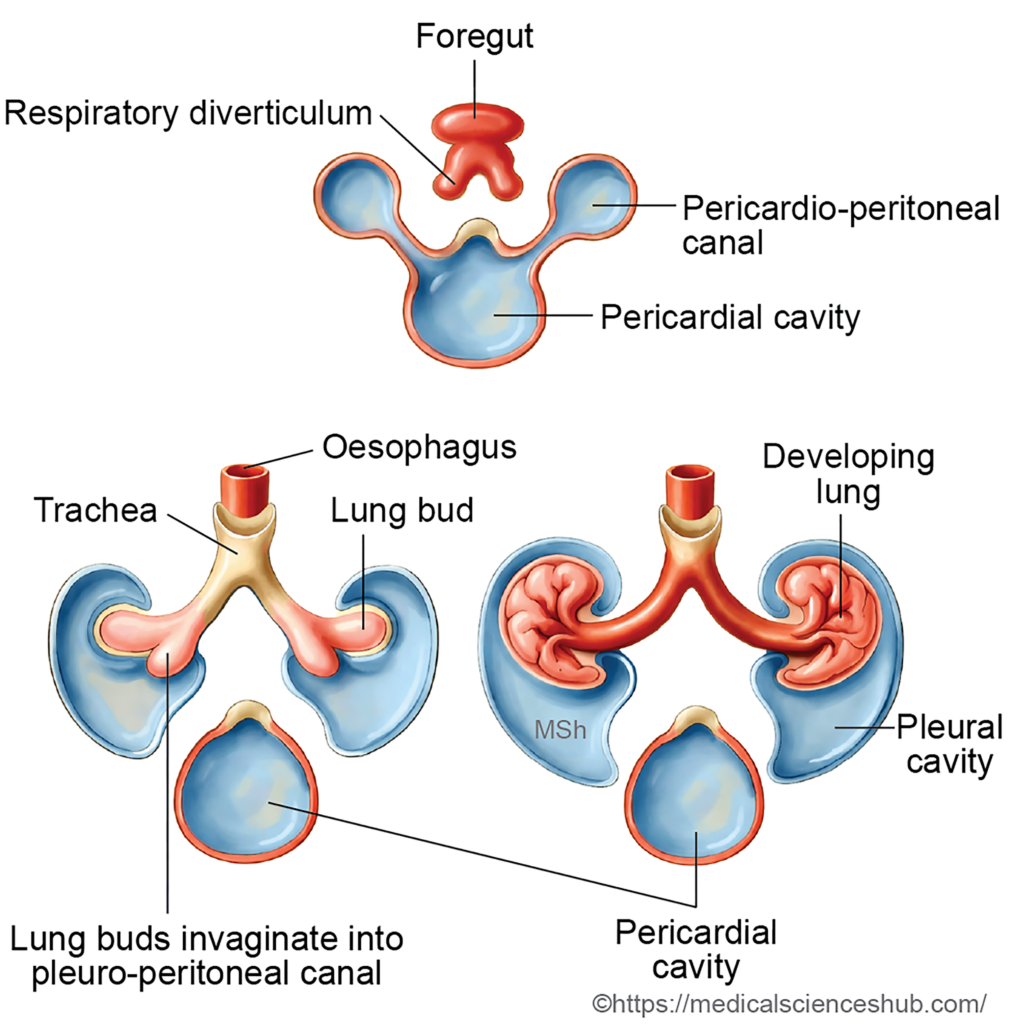
- The pleural cavities originate from the right and left pericardioperitoneal canals, which initially connect the pericardial cavity with the peritoneal cavity during early embryonic development.
Stages of Development
- Invagination stage
The lung buds, arising from the foregut, grow laterally and invaginate into the pericardioperitoneal canals. - Enlargement
As the lung buds increase in size, the pericardioperitoneal canals expand to accommodate the developing lungs. - Separation of cavities
Two folds derived from the somatopleuric mesoderm develop around the invaginating lung buds:- The pleuropericardial folds (membranes) grow medially and separate the pleural cavities from the pericardial cavity.
- The pleuroperitoneal folds (membranes) grow to separate the pleural cavities from the peritoneal cavity.
Both folds become continuous with the posterior margin of the septum transversum.
- Closure of the pleuropericardial openings
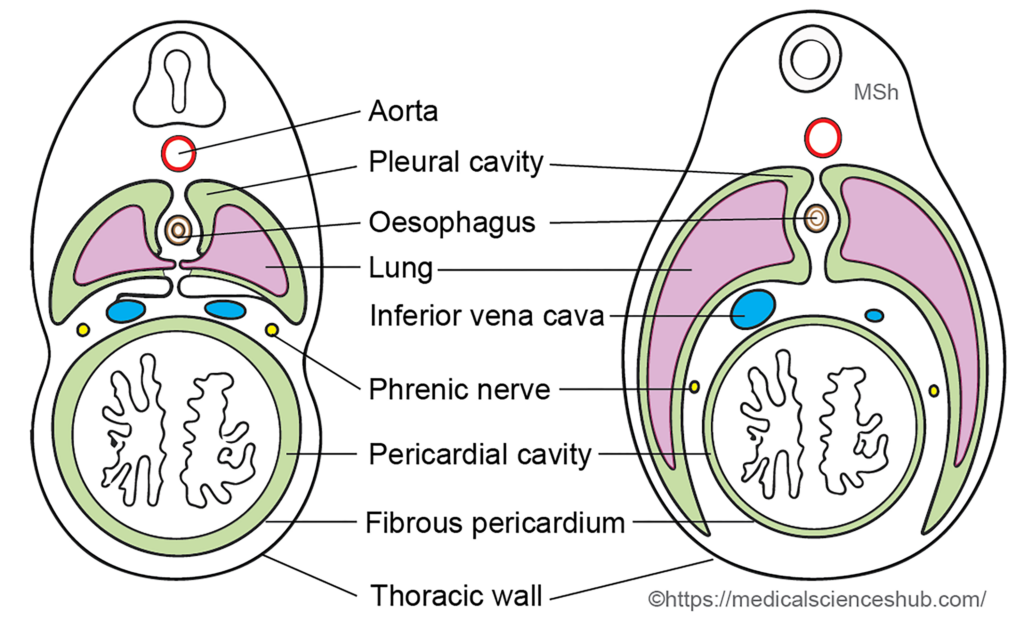
Around the sixth week, the pleuropericardial membranes (also called the pulmonary ridges of Mall) fuse with mesoderm surrounding the oesophagus, thereby separating the pleural and pericardial cavities. As the lungs enlarge, these membranes shift from an initially oblique position to a more vertical orientation. - Closure of the pleuroperitoneal openings
The pleuroperitoneal membranes grow ventrally and fuse with the septum transversum and adjacent mesodermal structures, closing the pleuroperitoneal canals and completing separation between the pleural and peritoneal cavities. - Expansion of the pleural cavities
Continued growth of the lungs causes expansion of the pleural cavities and contributes to the caudal displacement of the septum transversum. - Splitting of the body wall mesoderm
As the pleural cavities enlarge, the mesoderm of the body wall divides into two layers:- The outer layer, which contributes to the thoracic wall.
- The inner layer, which lines the pericardial cavity and forms the pleuropericardial membrane, later giving rise to the fibrous pericardium.
DEVELOPMENT OF PERITONEAL CAVITY
- The peritoneal cavity originates from the horseshoe-shaped limbs of the intraembryonic coelom.
- During embryonic folding, the lateral folds bring the right and left coelomic ducts toward the midline. Their fusion forms a single peritoneal cavity within the developing abdominal region.
- Initially, the peritoneal cavity communicates with the pericardial cavity through the pericardioperitoneal canals. As development proceeds, the formation of the pleural cavities and the growth of the septum transversum and pleuroperitoneal membranes separate the peritoneal cavity from the pleural cavities.
- Until approximately the 10th week of development, the peritoneal cavity remains in communication with the extraembryonic coelom at the umbilical ring. This connection allows the temporary physiological herniation of the midgut.
- The peritoneal layers arise from different components of the lateral plate mesoderm:
- The parietal peritoneum develops from the somatopleuric mesoderm.
- The visceral peritoneum develops from the splanchnopleuric mesoderm.
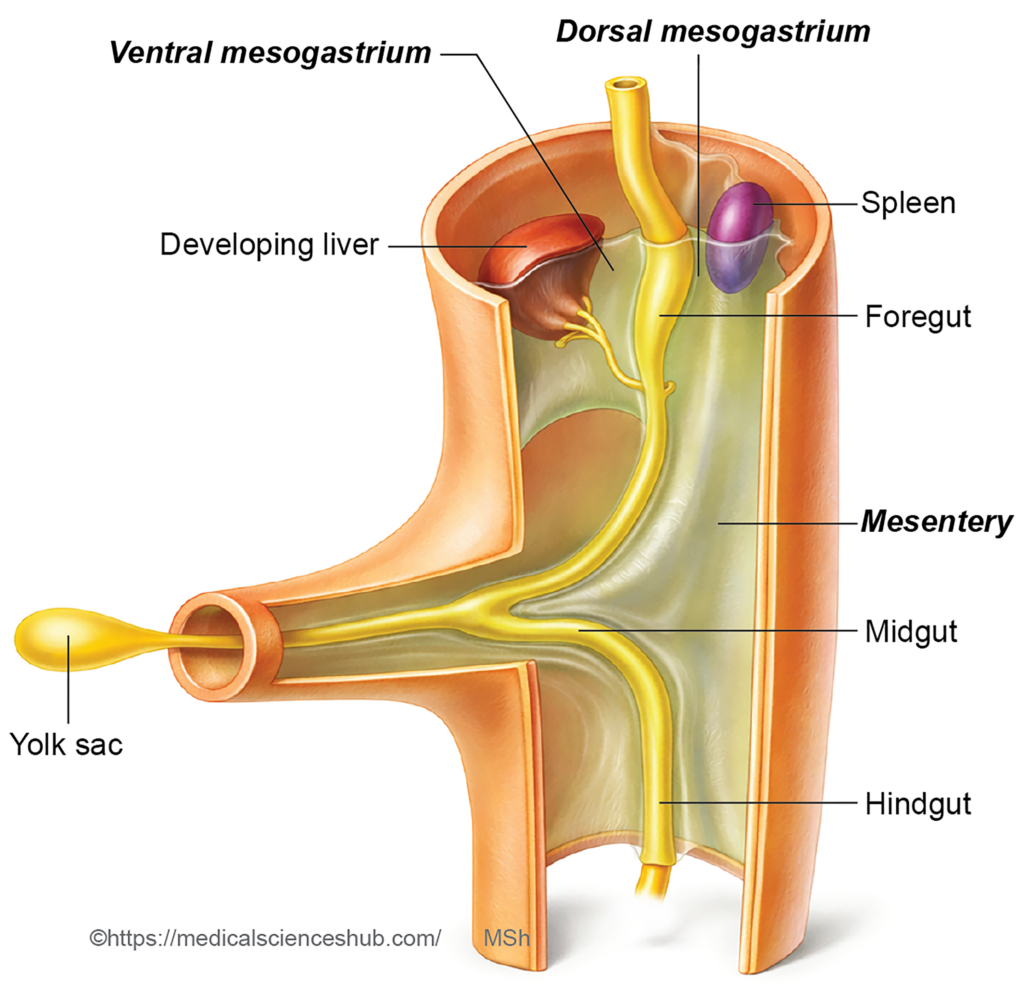
Formation Of Mesenteries
- Mesentery is a double-layered fold of peritoneum that suspends the abdominal viscera, particularly the intestine, from the body wall and provides a pathway for vessels, nerves, and lymphatics.
- Two primary types are recognized:
- Ventral mesentery: connects the gut tube to the anterior abdominal wall.
- Dorsal mesentery: connects the gut tube to the posterior abdominal wall.
- The ventral mesentery largely regresses during development and persists only in relation to:
- the caudal part of the oesophagus,
- the stomach, and
- the proximal part of the duodenum.
- In the region of the stomach, it is termed the ventral mesogastrium.
- With the formation of lateral body folds due to fusion of the splanchnopleuric mesoderm, the midgut and hindgut lose their ventral mesentery and retain only the dorsal mesentery. Subsequent gut rotation and zygosis (fusion of mesentery with the posterior abdominal wall) modify this dorsal mesentery to form definitive structures, including the mesentery of the jejunum and ileum, mesoappendix, transverse mesocolon, and sigmoid mesocolon.
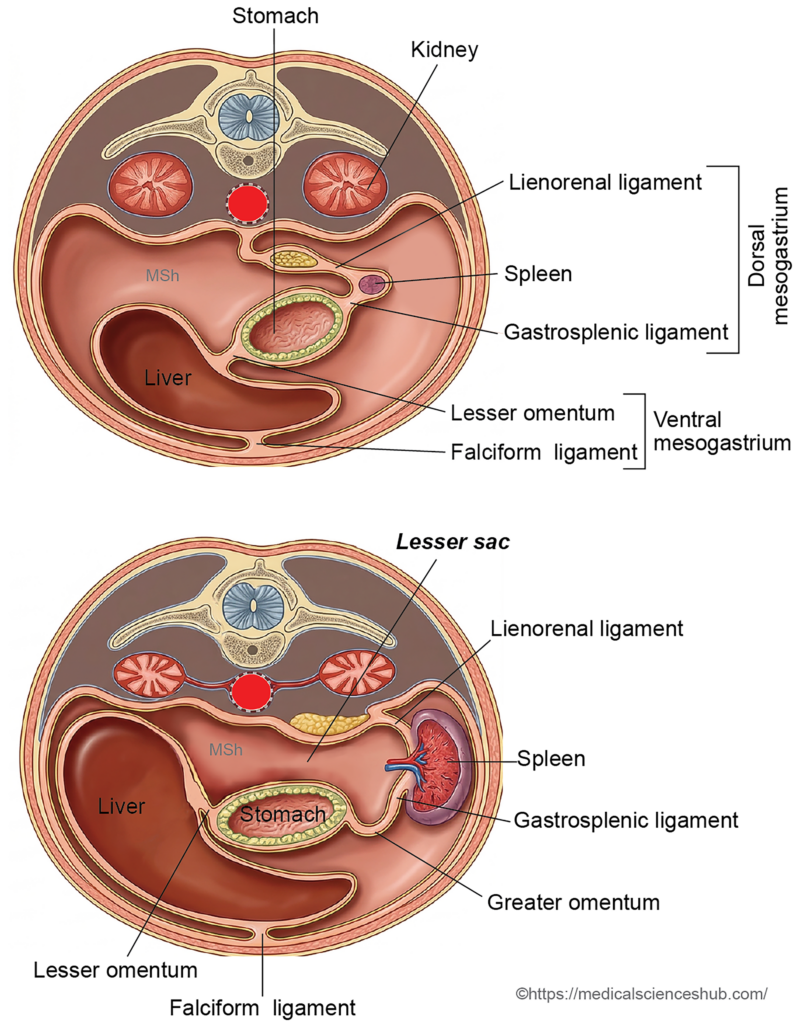
Development Of Lesser Sac
- The lesser sac (also termed the omental bursa) is a subdivision of the peritoneal cavity located posterior to the stomach and the lesser omentum.
Development
1. Formation of the dorsal mesogastric recess
- Small spaces, termed pneumoenteric recesses, appear within the dorsal mesogastrium.
- The left recess regresses early, whereas the right recess enlarges and communicates with the peritoneal cavity.
- This expanding right recess extends behind the stomach to form the main part of the lesser sac. Its upward extension behind the liver forms the superior recess. A transient cranial extension above the diaphragm, called the infracardiac bursa, usually disappears.
2. Formation of the vestibule
- Rotation of the stomach and growth of the liver reposition part of the peritoneal cavity behind the lesser omentum (derived from the ventral mesogastrium).
- This region forms the vestibule of the lesser sac.
3. Formation of the inferior part
- Rotation of the stomach and development of the spleen divide the dorsal mesogastrium into the gastrosplenic ligament and lienorenal ligament.
- The portion of the lesser sac extending between these ligaments forms the splenic recess.
DEVELOPMENT OF DIAPHRAGM
- The diaphragm is a musculotendinous partition that separates the thoracic cavity from the abdominal cavity. It consists of a central tendon and muscular portions, including the crura. Its development involves contributions from several embryonic structures.
Components and their embryological origins
- The central tendon is primarily formed from the pleuroperitoneal membranes.
- The crura of the diaphragm develop from the dorsal mesentery of the oesophagus.
- The muscular component arises from myoblasts derived from cervical somites (C3–C5), which migrate into the developing diaphragm.
- The ventrolateral peripheral portion develops from the mesoderm of the lateral body wall.
Earlier descriptions suggested that the central tendon developed mainly from the septum transversum; however, current understanding emphasizes significant contribution from the pleuroperitoneal membranes during diaphragm formation.
Stages in the Development of the Diaphragm
- Septum transversum
The septum transversum initially forms a thick mass of mesoderm positioned between the thoracic and peritoneal cavities. It contributes to the early partition separating these cavities and serves as an important scaffold for later diaphragm development. - Contribution of pleuroperitoneal membranes
The right and left pleuroperitoneal membranes grow medially to close the pleuroperitoneal canals, thereby separating the pleural cavities from the peritoneal cavity. These membranes contribute significantly to the formation of the central tendon of the diaphragm.- Note: Cervical somites (C3–C5) give rise to myogenic precursor cells that migrate into the pleuroperitoneal folds. As these folds extend across the septum transversum, they carry the migrating cells, which later differentiate into the muscular components of the diaphragm.
- Contribution of the dorsal mesentery of the oesophagus
The dorsal mesentery of the oesophagus forms the crura of the diaphragm, which anchor the diaphragm to the vertebral column. - Contribution of the lateral body wall
Expansion of the pleural cavities divides the lateral body wall mesoderm into outer and inner layers. The outer layer forms the definitive thoracic wall, whereas the inner layer grows inward to form the ventrolateral muscular part of the diaphragm, peripheral to the region derived from the pleuroperitoneal membranes.

Descent of the Septum Transversum
- During the fourth week of development, the septum transversum is located in the cervical region at the level of the third, fourth, and fifth cervical somites. These segments later contribute to the phrenic nerve (C3–C5), which becomes the primary motor nerve of the diaphragm.
- As the embryo grows, particularly with the development of the heart and the expansion of lung buds within the pericardioperitoneal canals, the diaphragm gradually shifts downward. By approximately the sixth week, it reaches its definitive thoracoabdominal position, corresponding roughly to the T7–T12 vertebral levels.
- During this descent, the diaphragm retains its original innervation. Consequently, the phrenic nerve descends with the diaphragm to maintain its neural connection.
Factors Contributing to the Descent of the Diaphragm
Several developmental changes contribute to the caudal displacement of the diaphragm:
- Elongation of the neck region associated with the growth of the pharyngeal arches.
- Expansion of the pleural cavities as the lungs enlarge.
- Progressive growth and repositioning of the heart within the thoracic cavity.
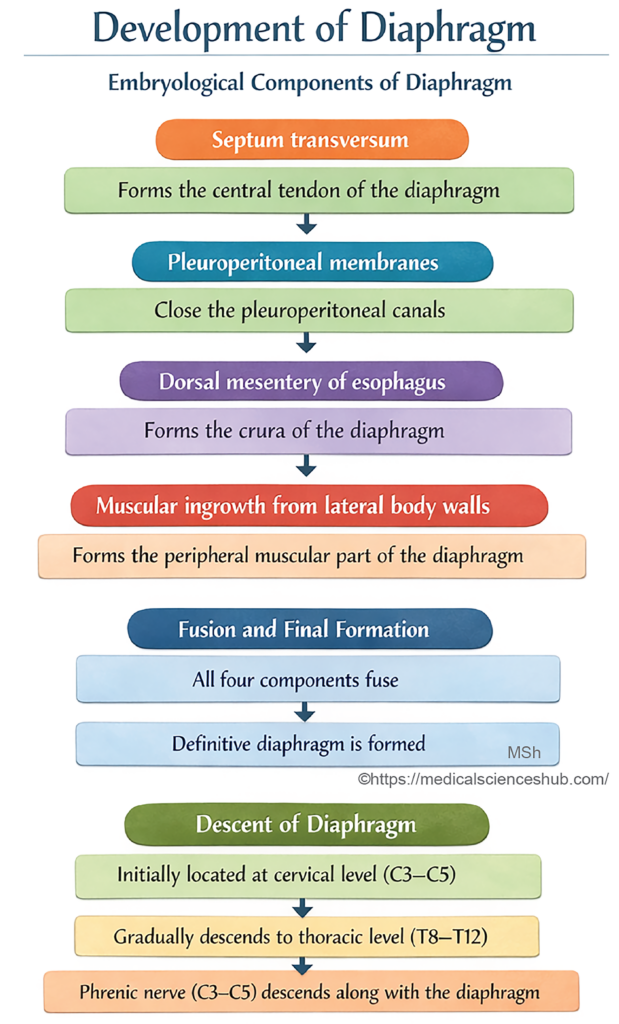
Table 16.1: Embryological Origin of the Diaphragm
| Component | Embryological Source | Key Point |
|---|---|---|
| Central tendon | Septum transversum | Forms non-muscular center; descends from cervical to thoracic region |
| Right & left crura | Dorsal mesentery of oesophagus | Form lumbar attachments and oesophageal hiatus |
| Muscular part | Cervical somites (C3–C5) | Myoblast migration; basis of phrenic nerve supply |
| Peripheral part | Lateral body wall mesoderm | Forms outer muscular rim with body wall expansion |
CLINICAL EMBRYOLOGY
Congenital Anomalies of diaphragm
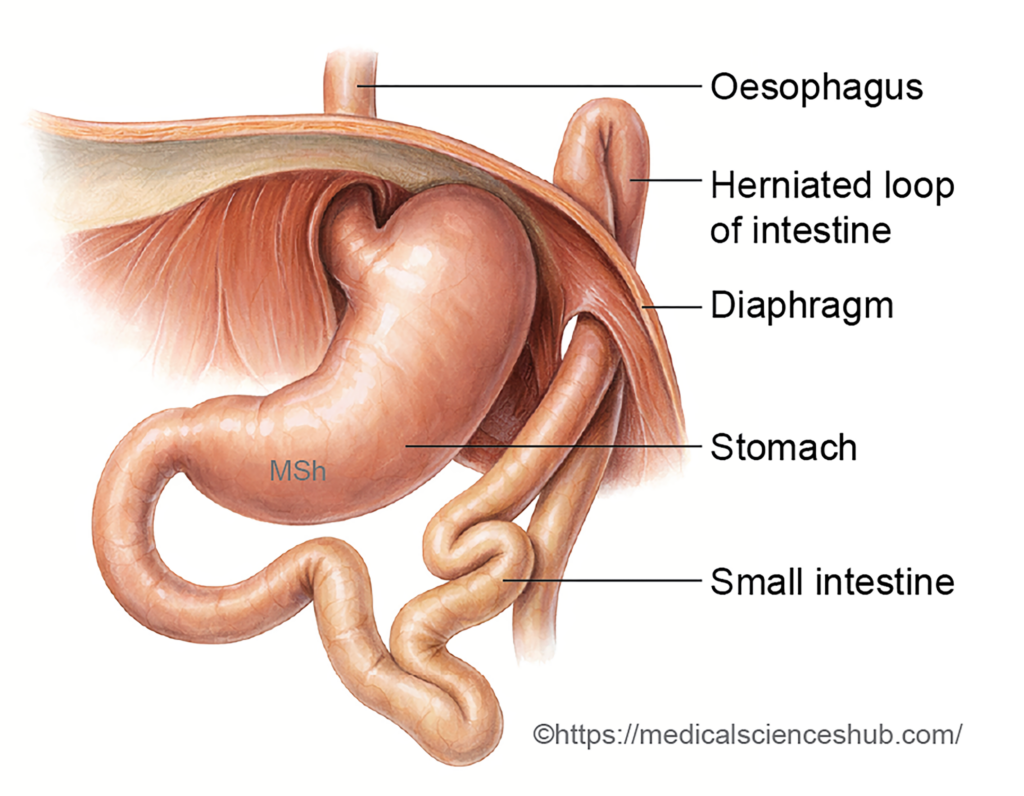
- Retrosternal (parasternal) hernia
In this anomaly, abdominal contents protrude through the foramen of Morgagni, a gap between the sternal and costal parts of the diaphragm, allowing viscera to enter the anterior thoracic cavity. - Eventration of the diaphragm
Eventration refers to an abnormal elevation of one dome of the diaphragm due to incomplete muscular development. The affected region becomes thin and membranous, permitting abdominal organs to bulge into the thoracic cavity, although the diaphragm remains intact.
Congenital Diaphragmatic Hernia (CDH)
Congenital diaphragmatic hernia is the protrusion of abdominal contents into the thoracic cavity resulting from defective formation of the diaphragm. This condition is clinically significant because it often causes pulmonary hypoplasia, making it a life-threatening disorder in newborns.
- Incidence: approximately 1 in 2000 births.
- Major complication: severe pulmonary hypoplasia leading to respiratory distress, the most common cause of mortality.
- Characteristic clinical features: breathlessness, cyanosis, and an unusually scaphoid (flat) abdomen.
- Genetic association: microdeletion involving chromosome 15q26.
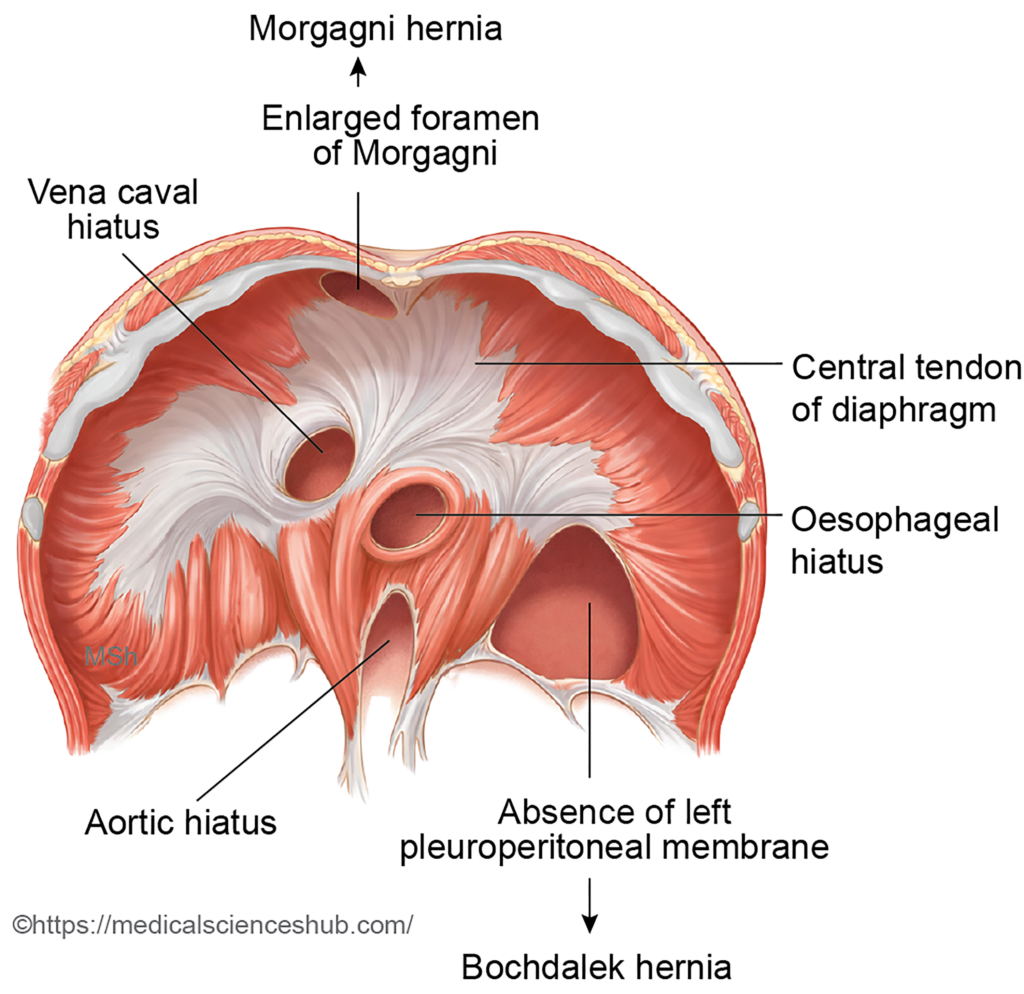
Classification of CDH
- Bochdalek hernia (posterolateral hernia)
- Represents about 95% of CDH cases.
- Caused by failure of the pleuroperitoneal membrane to close the pleuroperitoneal canal.
- Occurs predominantly on the left side (about 85–90%).
- Morgagni hernia
- Also called retrosternal or parasternal hernia.
- Results from herniation of abdominal viscera through the foramen of Morgagni, usually in the anterior right portion of the diaphragm.
- Diaphragmatic eventration
- Characterized by abnormal elevation of the diaphragmatic dome due to paralysis, aplasia, or atrophy of diaphragmatic muscle fibers.
Important Questions
- Describe the embryological development of the diaphragm.
- Explain congenital diaphragmatic hernia, including its developmental basis and clinical significance.
- Describe the formation and development of the lesser sac (omental bursa).
