Competencies
- AN43.4: Describe the development and developmental basis of congenital anomalies of pituitary gland and thyroid gland. Note: No specific competency is given for endocrine glands.
INTRODUCTION
- Endocrine glands, also known as ductless glands, release hormones directly into the bloodstream. These hormones travel via circulation to target organs, where they bind to specific receptors to produce targeted effects.
- The primary endocrine glands include the pituitary, pineal, thyroid, parathyroid, adrenal glands, pancreatic islets of Langerhans, testes, ovaries, and hypothalamus. The hypothalamus regulates anterior pituitary secretions, among its other roles.
PITUITARY GLAND (HYPOPHYSIS CEREBRI)
- The pituitary gland, an unpaired endocrine gland, lies within the sella turcica, a bony depression in the sphenoid bone. It comprises two main parts: the adenohypophysis (anterior pituitary) and neurohypophysis (posterior pituitary).
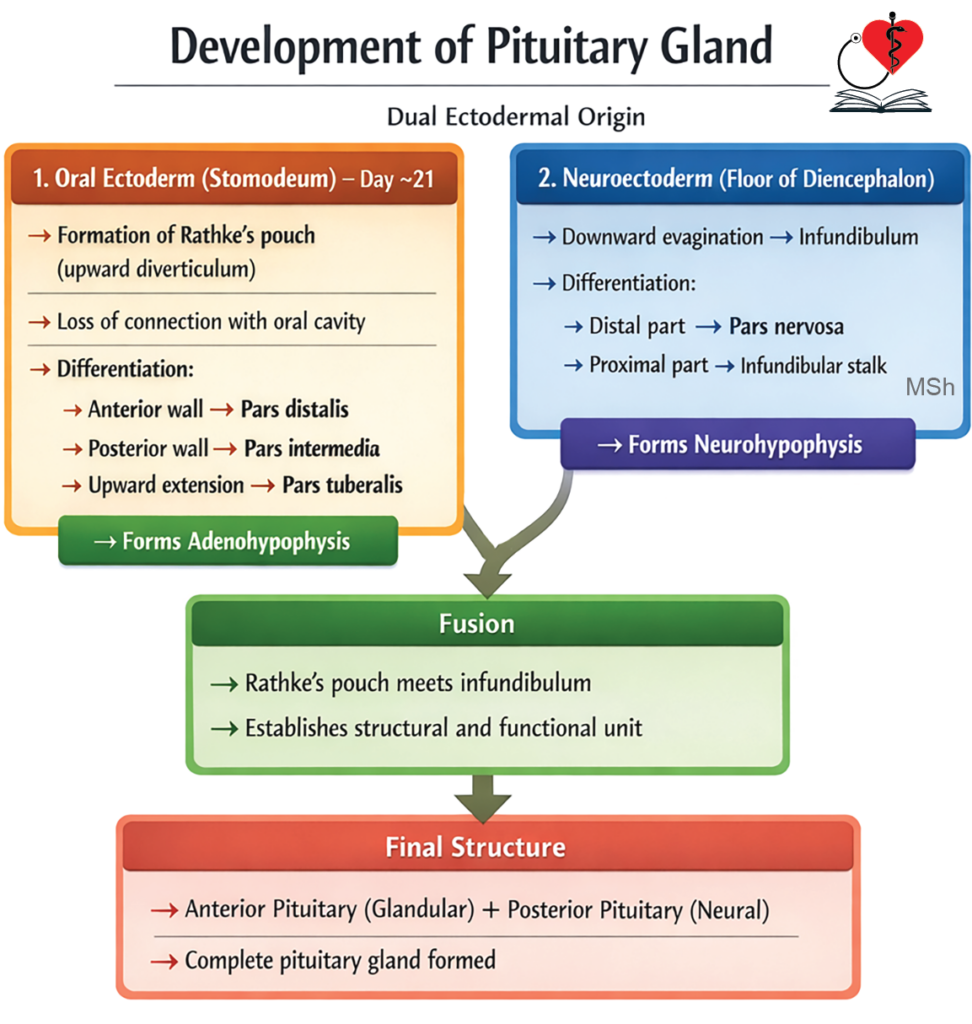
- The adenohypophysis derives from Rathke’s pouch, an ectodermal outgrowth of the stomodeum. This anterior portion includes the pars distalis, pars intermedia, and pars tuberalis, with Rathke’s pouch remnant forming an intraglandular cleft. The neurohypophysis arises from an evagination of the third ventricle floor in the diencephalon.
Stages of Development
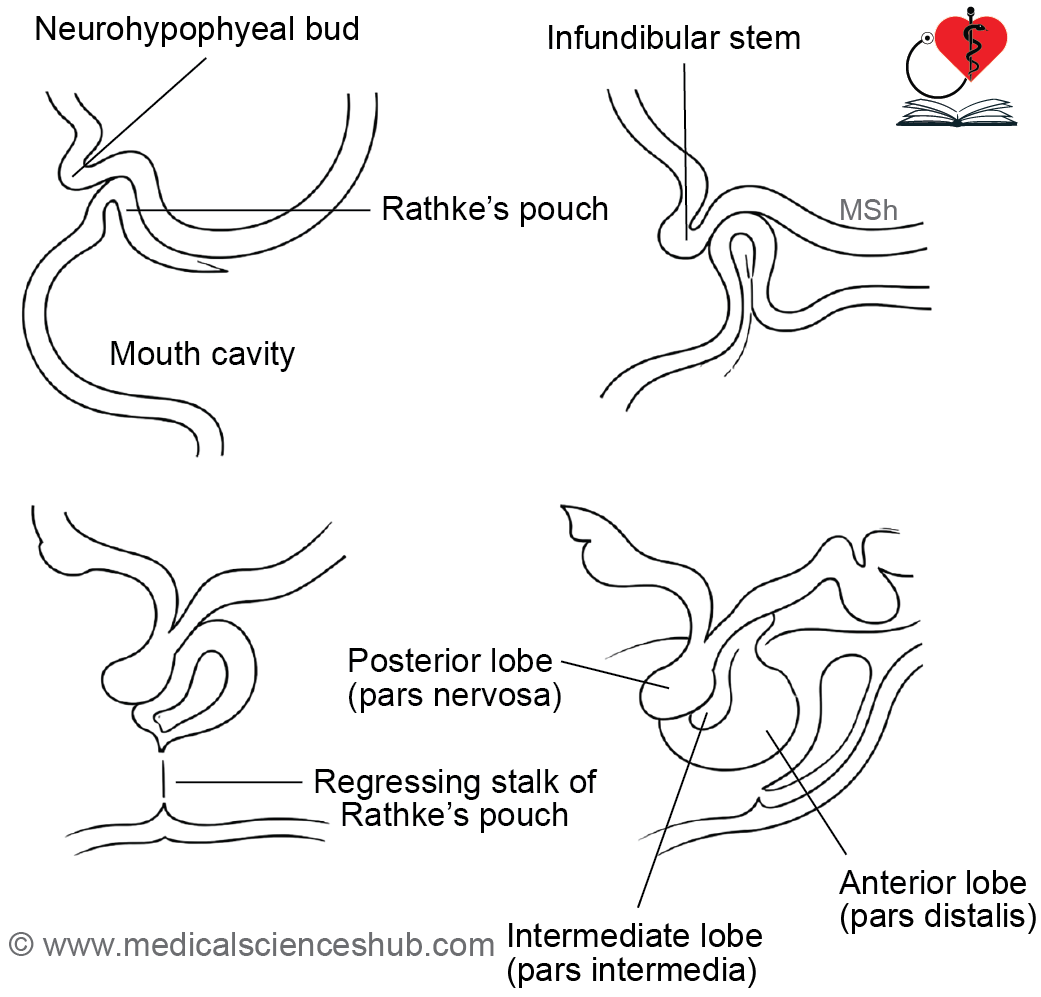
- The adenohypophysis forms from Rathke’s pouch. On day 21 of intrauterine life, ectoderm of the stomodeum thickens, invaginates toward the diencephalon, and creates Rathke’s pouch. By the second month, this pouch detaches from the stomodeum. Cells in its thick anterior wall proliferate into the pars distalis, while the thin posterior wall forms the pars intermedia; the pouch cavity becomes an intraglandular cleft, and upward anterior growth yields the pars tuberalis.
- The neurohypophysis derives from the infundibular process of the diencephalon. In the sixth week of intrauterine life, this process evaginates from the third ventricle floor, extends toward Rathke’s pouch, and fuses with it to form the pars nervosa. The stalk linking pars nervosa to the hypothalamus develops into the infundibulum.
Histogenesis
Histogenesis of the pituitary begins in the fourth month of intrauterine life. In the adenohypophysis, acidophils appear first, followed by basophils and chromophobes. In the neurohypophysis, neuroglial cells emerge by the fourth month, with subsequent axonal growth from the hypothalamic supraoptic and paraventricular nuclei.
Figure 21.1a: Development of pituitary gland (Click to see figure)
CLINICAL EMBRYOLOGY
Developmental Anomalies of the Pituitary Gland
- Craniopharyngiomas arise from Rathke’s pouch remnants in the craniopharyngeal canal. As Rathke’s pouch migrates from the stomodeum to the sella turcica, residual cells in this canal or near the sphenoid bone in the nasopharynx roof can form these tumors. They manifest in children aged 5–14 years or adults aged 50–70 years.
- An accessory pituitary gland, or pharyngeal hypophysis, may occur along the posterior nasopharyngeal wall.
- Pituitary agenesis or hypoplasia represents another possible congenital anomaly.
ADRENAL GLAND
- The adrenal glands (or suprarenal glands) are paired glandular masses situated at the superior pole of each kidney. Each gland features a superficial cortex and central medulla.
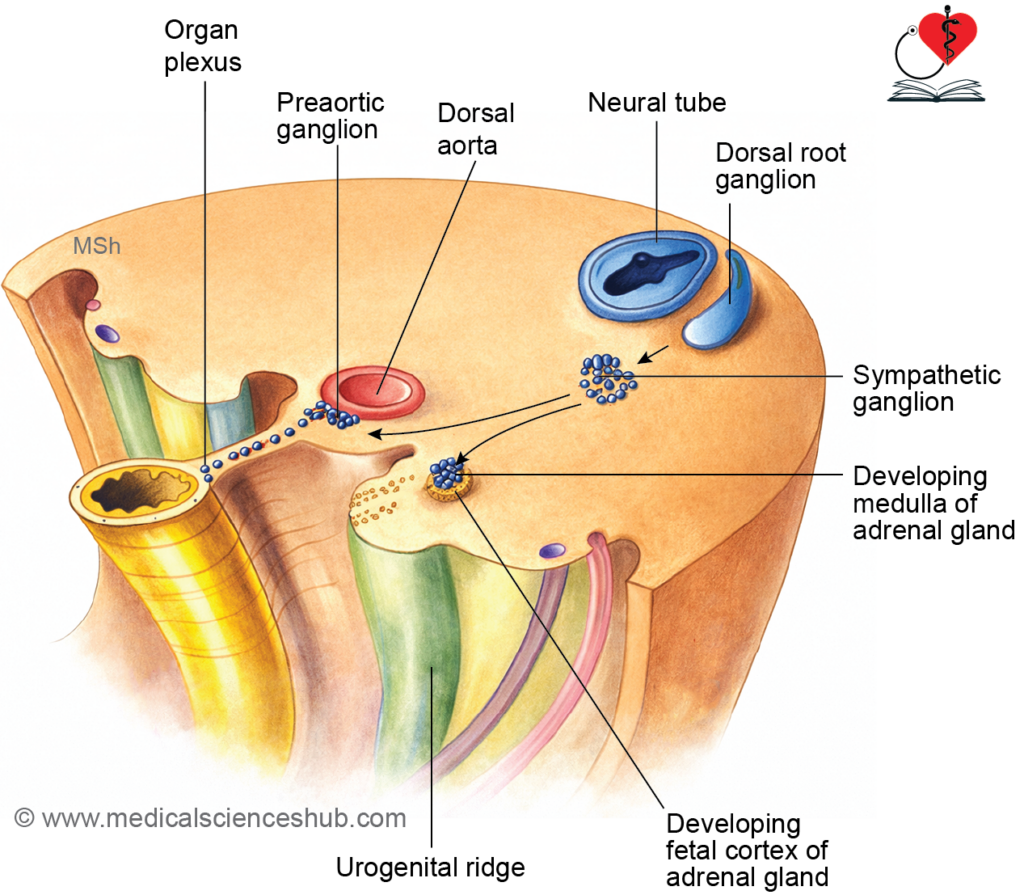
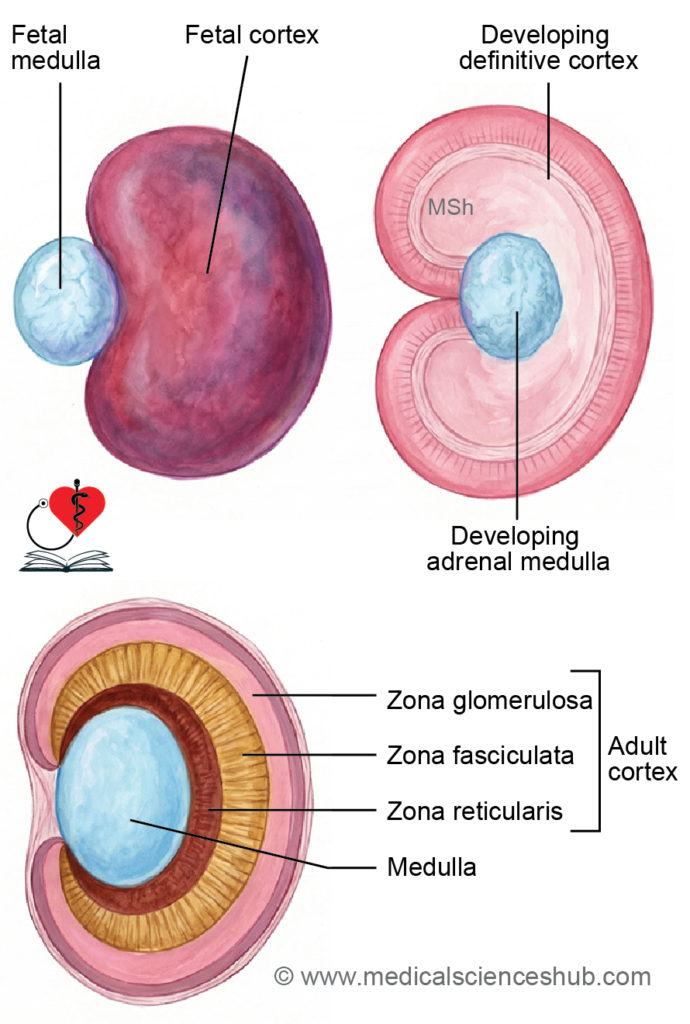
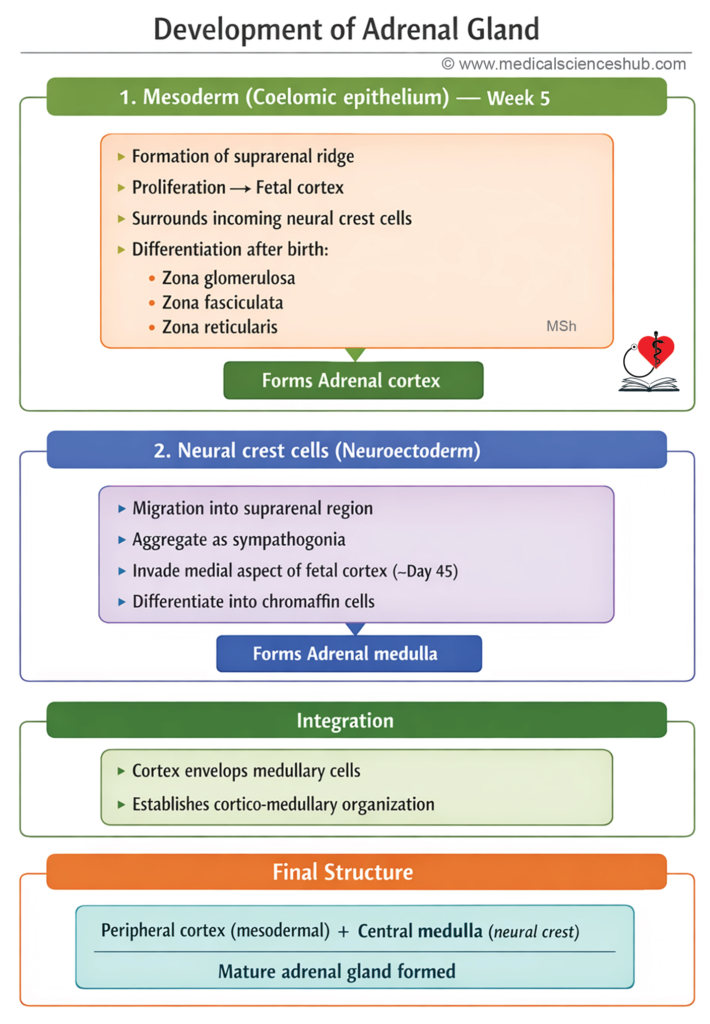
- The adrenal cortex originates from mesodermal coelomic epithelium, which forms the suprarenal ridge. An initial provisional cortex later gives way to the definitive cortex, differentiating into the zona glomerulosa, zona fasciculata, and zona reticularis.
- The adrenal medulla develops from neural crest-derived sympathochromaffin cells.
Stages of Adrenal Gland Development
- The adrenal cortex derives from mesoderm, while the adrenal medulla originates from neural crest cells (neuroectodermal).
Adrenal Cortex Development
- In the fifth week of intrauterine life, coelomic epithelium near the developing gonad proliferates to form the suprarenal ridge. By the second month, this ridge produces acidophilic cells around the primitive medulla, creating the fetal cortex. In the third month, a second layer of small basophilic cells from the ridge encases the fetal cortex to form the definitive cortex.
Adrenal Medulla Development
- By day 45 of gestation, sympathogonia from neural crest accumulate near fetal cortical cells, invade them, and organize into clusters and cords. These differentiate into medullary cells. Preganglionic sympathetic neurons synapse with these cells, which function like postganglionic neurons.
Postnatal Changes
- Fetal adrenals are proportionally 10–20 times larger than adult glands, with the cortex comprising only 15–20% of the parenchyma. The fetal cortex regresses fully by age two, reducing overall size; zona reticularis emerges by the end of the third year. At birth, only zona glomerulosa and zona fasciculata are present.
CLINICAL EMBRYOLOGY
Congenital Anomalies of adrenal gland
- Ectopic adrenal tissue may occur beneath the renal capsule or fuse with the kidney or liver.
- Congenital adrenal hyperplasia (CAH), most commonly from 21-hydroxylase deficiency, impairs cortisol and aldosterone synthesis, leading to androgen excess. In males, this triggers precocious puberty, termed adrenogenital syndrome. In females, it enlarges the clitoris, resulting in female pseudohermaphroditism.
Development of Thyroid Gland
The thyroid gland develops from two embryological sources:
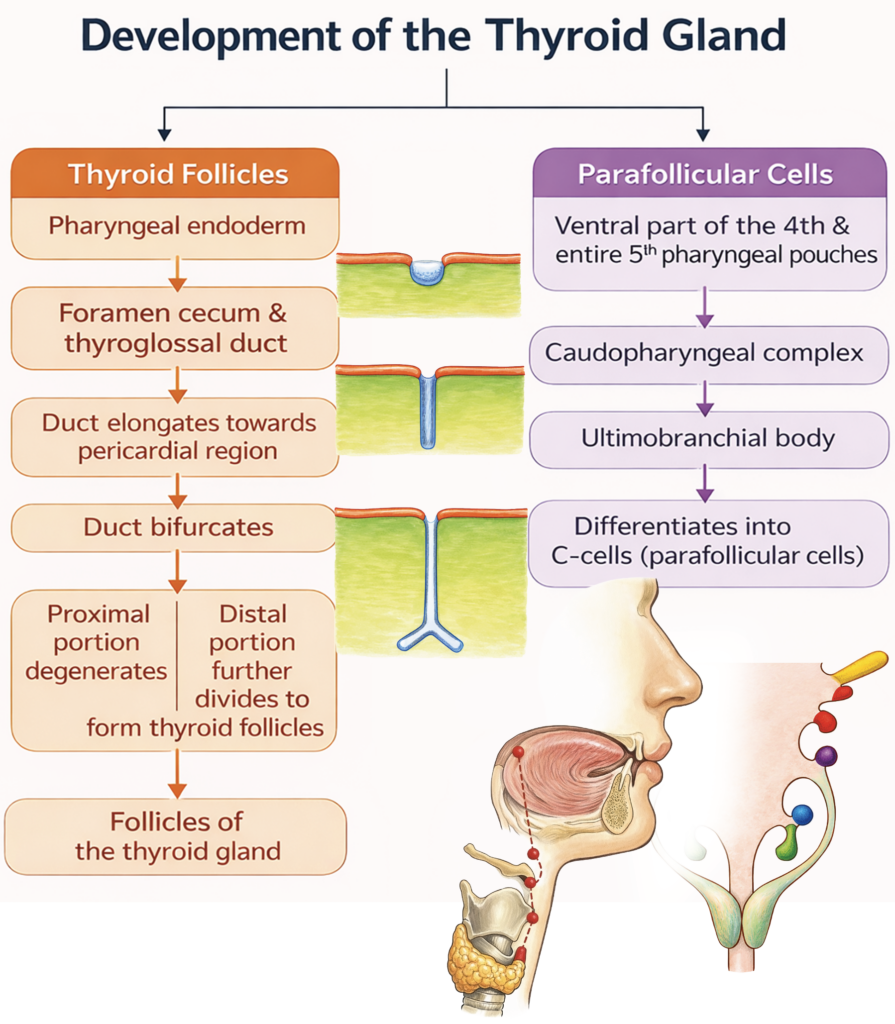
- Follicular cells arise from a midline endodermal thickening that forms the thyroglossal duct.
- Parafollicular (C) cells originate from the ultimobranchial body, which is derived mainly from the fourth (and rudimentary fifth) pharyngeal pouch complex.
The thyroid is the first endocrine gland to begin development in the embryo. By the end of the first trimester (around the 10th–12th week), the follicular cells begin producing thyroid hormones.
Stages of Development
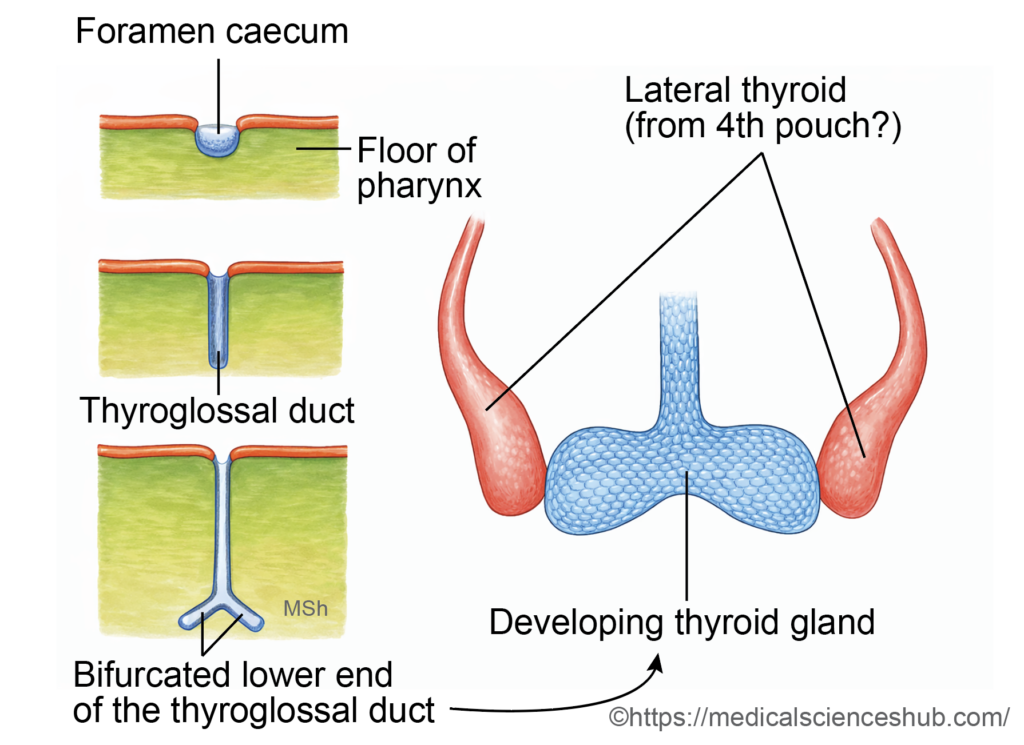
- In the floor of the primitive pharynx, a midline swelling called the tuberculum impar appears between the first and second pharyngeal arches.
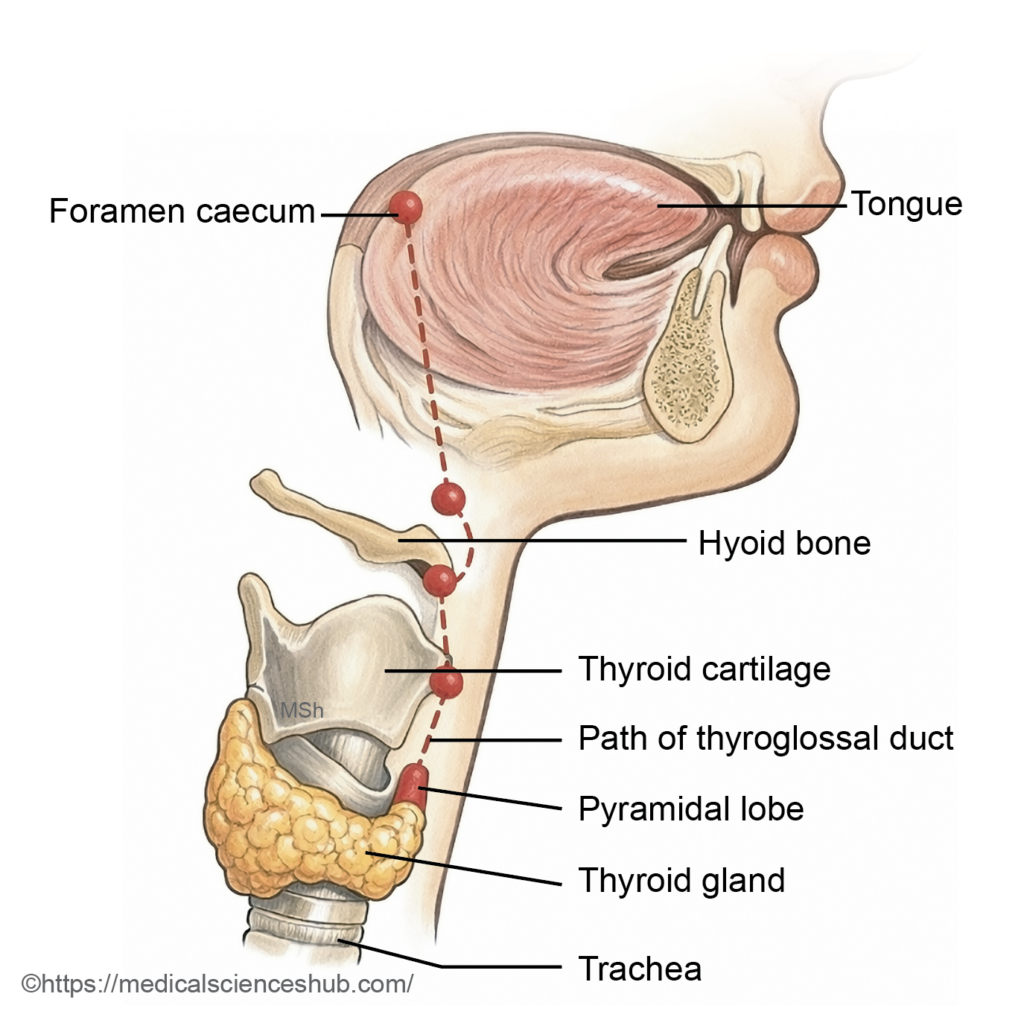
- Around the 24th day of development, an endodermal thickening just posterior to this region forms a median diverticulum known as the thyroid primordium. Its opening in the tongue persists as the foramen cecum.
- The primordium elongates inferiorly as the thyroglossal duct, descending in the midline anterior to the developing hyoid bone and laryngeal cartilages.
- By the seventh week, the distal end enlarges and divides to form the right and left lobes of the thyroid gland. The thyroglossal duct normally degenerates thereafter.
- The ultimobranchial bodies later fuse with the developing thyroid and contribute parafollicular (C) cells, which secrete calcitonin.
This coordinated migration and differentiation establish the final position and cellular composition of the thyroid gland in the anterior neck.
CLINICAL EMBRYOLOGY
Anomalies of the Thyroid Gland
- Pyramidal Lobe: A pyramidal lobe is an accessory projection of thyroid tissue that may arise from the isthmus or from either lateral lobe. Its size and length are variable. It represents a persistent remnant of the thyroglossal duct.
- Congenital Hypothyroidism: Congenital hypothyroidism may result from:
- Athyreosis (complete absence of the thyroid gland),
- Thyroid ectopia (abnormal location),
- Thyroid hypoplasia (underdevelopment), or
- Dyshormonogenesis, caused by genetic defects affecting thyroid hormone synthesis.
- Early detection is essential to prevent impaired physical growth and neurodevelopment.
- Thyroid Ectopia: It refers to abnormal positioning of the gland along the developmental pathway of the thyroglossal duct. The most common site is a lingual thyroid at the base of the tongue.
- Ectopic Thyroid Tissue: Ectopic thyroid tissue may also occur outside the normal migratory pathway. Reported sites include the larynx, trachea, esophagus, mediastinum, and, rarely, the ovary (as part of a teratoma, e.g., struma ovarii).
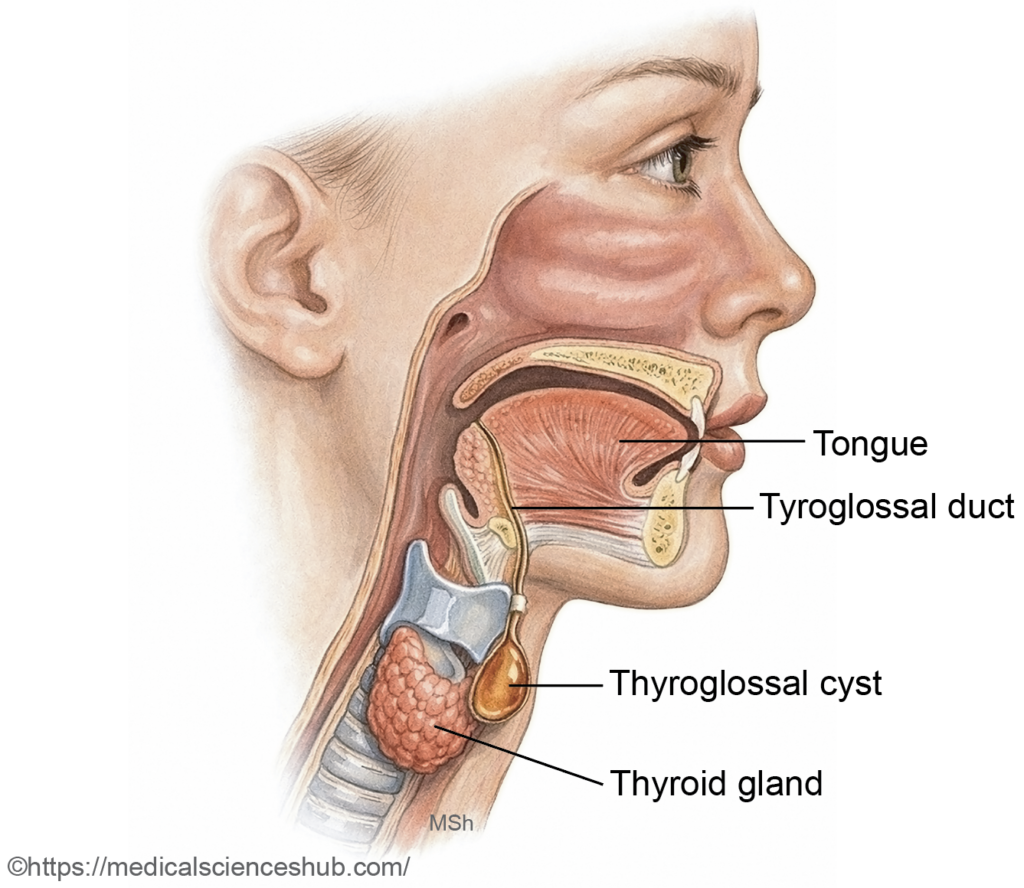
- Thyroglossal cyst and fistula
- The thyroid gland develops from a midline endodermal diverticulum that descends as the thyroglossal duct, which normally undergoes degeneration. Persistence of any ductal segment may lead to a thyroglossal cyst, typically presenting as a painless, midline neck swelling that moves with swallowing and tongue protrusion.
- If the cyst becomes infected or ruptures externally, a persistent tract may form a thyroglossal fistula. Rarely, malignant transformation may occur within a thyroglossal cyst.
Important Questions
- Write a short note on the development of adrenal gland.
- Write a short note on the pituitary gland.
- Write a short note on the development of thyroid gland and its developmental anomalies.
